The issue of LDL and total mortality risk is cloudy at best. Many of the benefits of statins may be independent of its lipid lowering and more a consequence of its anti inflammatory component, in which case aren’t there safer anti inflammatories out there?
Your idea of low dose and infrequent use might be a good compromise for statins.
1 Like
RE, Anti-inflammatory:
I take Boswellia Serrata (Frankincense) because I have a knee that I tweaked years ago playing tennis. Nothing I did seemed to make it better. Then I read some anecdotal reports of its efficacy in relieving knee pain. It was a near miracle for me. After taking it for a few months my knee problems completely disappeared and I have had no problems since. I continue to take it because of its anti-inflammatory properties. As I grow older I think anti-inflammatory supplements are more important than anti-oxidants. I think it is extremely interesting that while Boswellia Serrata treats OA in general it seems to target the knees.
A pilot, randomized, double-blind, placebo-controlled trial to assess the safety and efficacy of a novel Boswellia serrata extract in the management of osteoarthritis of the knee
BSE also significantly reduced the serum levels of high-sensitive C-reactive protein, a potential inflammatory marker associated with OA of the knee.
1 Like
desertshores,
What dose did you take for your knees?
As with all supplements, all brands are not equal in potency. Depending on the brand, I take 2 - 4 grams of the extract. The extract comes in several potencies and forms. I really don’t know which brand is best. I would stick with one of the brands you trust.
Check out “Knees over toes guy” on YouTube & IG. Very low impact exercises that fixed my knees.
2 Likes
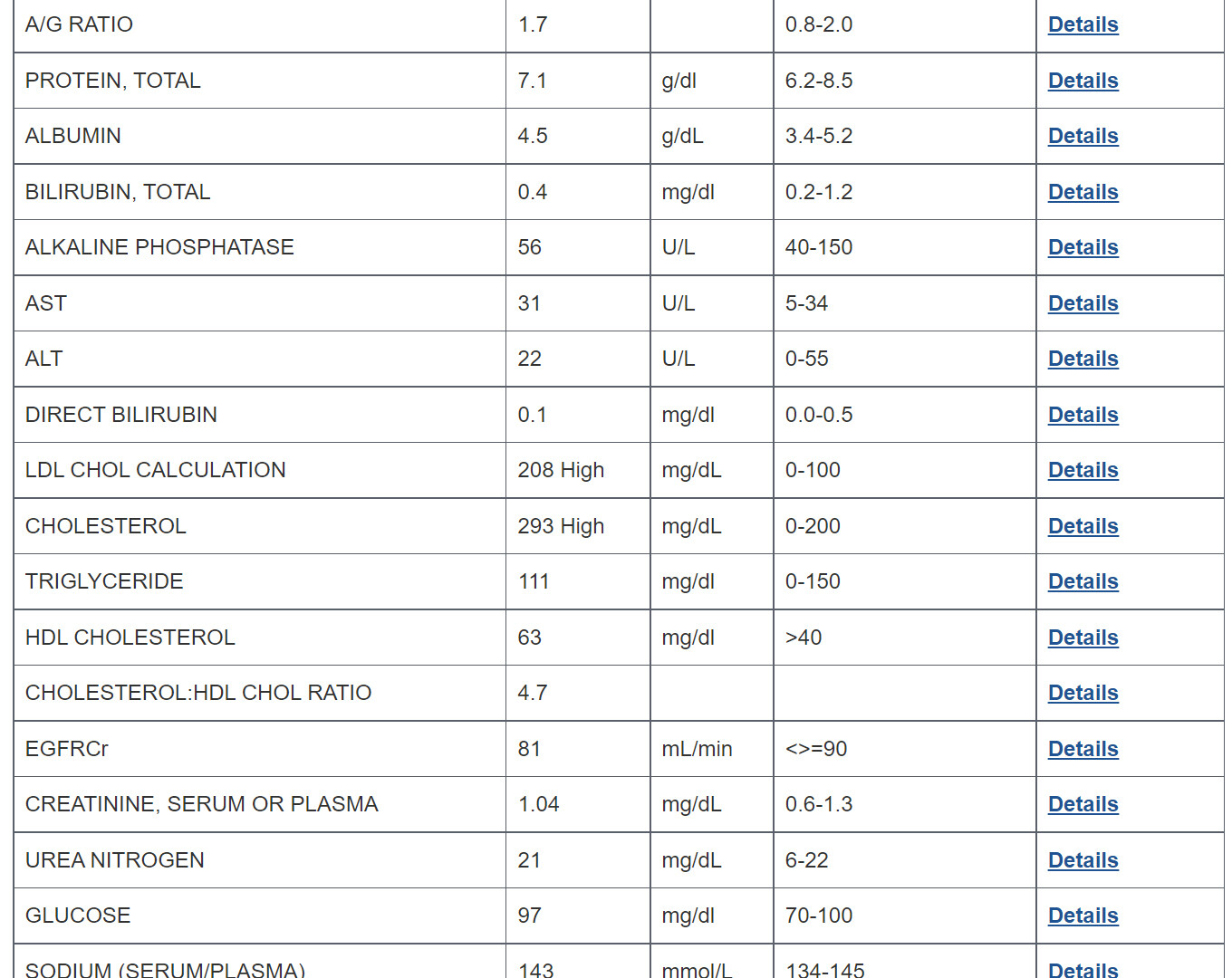
So I just had my annual bloodwork done, and my total cholesterol and LDL are both determined to be high. (see below) The doc is prescribing a daily dose of 1/2 of a 40 mg tab of Rosuvastatin. My question is, how much of that tab do I want to take for the anti-aging and life extension effects without suffering from any side effects? Or should I just take the entire 20 mg dose?
I’ll leave the docs to comment on the statin, but from strictly a lipids risk:
TG HIGH
TG/HDL = 1.76 (my target is < 1)
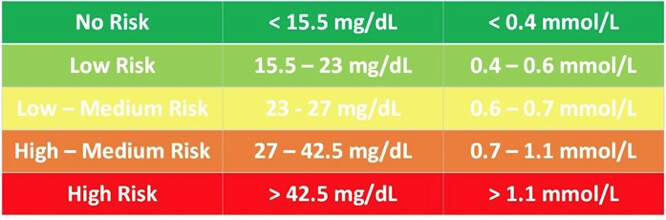
Remnant Cholesterol (RC) = TC-LDL-HDL = 22 (LOW-MEDIUM)
What’s your diet, A1C, BMI? No APOB I assume?
Do you have a CAC?
RC risk summary:
I never did a coronary artery calcium score, and I’m not sure if the US Department of Veterans Affairs covers that, but I’ll check.
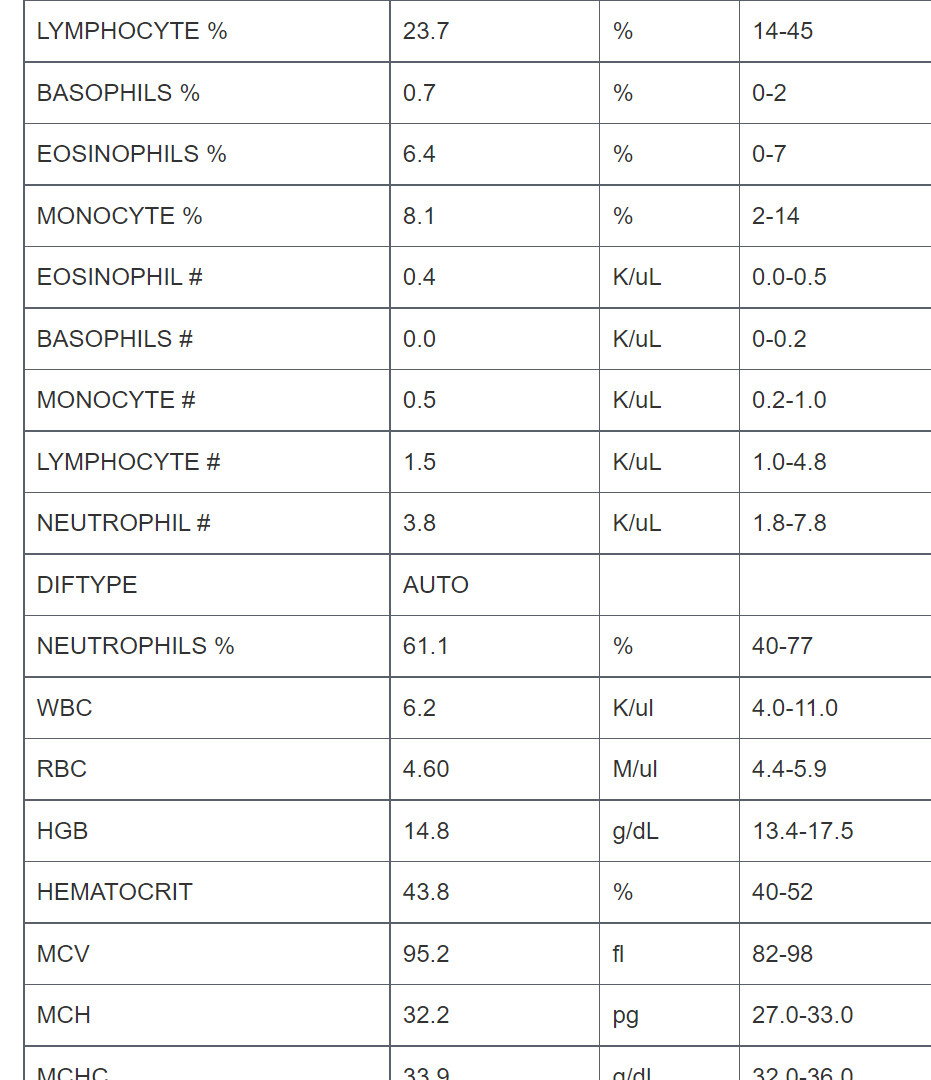
I didn’t find an entry for A1C but maybe this will help:
My BMI is 24, and my diet is pretty spot on. I should mention that I’ve been on .8 cc of Testosterone Cypionate weekly for the past 4 years, which I know raises blood pressure and cholesterol numbers, unfortunately.
No HbA1c, your 3 month average blood glucose…would be an indication of your metabolic dysregulation status.
Get a CAC, however which way.
What does “diet is pretty spot on” mean? % protein/fat/carbs, types of fats and carbs and proteins?
My TRT hasn’t impacted my lipids…my diet is the main manipulative lever.
You have before/after TRT blood panel, no other interventions?
What about BP?
1 Like
Evidence in mice does not support low-dose simvastatin, for maximal lifespan. Low-dose sim mice lived to about 1210 days, versus 1250 for controls. It is the high-dose mice who lived longer (1360 sim versus 1250 control)…
With regard to median lifespan, there is a negligible swerve to the right of the chart of sim mice (low and high does) versus controls.
As earlier posted by Jay, you can find charts of all tested substances below:
Absent are OTC products meclizine and astaxanthin, mentioned at 8:12 of the Joe Cohen video. Results of the two are awaiting publication.
2 Likes
Mice don’t normally get ischemic heart attacks from atherosclerosis. Heck, even chimps basically don’t get them:
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1752-4571.2008.00064.x
Again and again, one needs context when interpreting literature. While statins aren’t proven to prevent heart attacks in those who aren’t clearly indicated for them based on traditional ASCVD scoring, maximal lifespan interventions are only good if you can actually live to see them. That means one needs to have the best possible information to play your hand in risk stratification and making decisions (or a decision not to intervene).
It is plausible statins could increase the maximal lifespan in humans and even more so if some intervention does end up slowing or reversing atherosclerosis (the disease process starts in teenager years and most older adults have some stage of atherosclerosis after about 50 years later on average that doesn’t necessarily show up as a heart attack or stroke but is contributed or caused by atherosclerosis such as dementia with a cerebrovascular factor) - it is plausible that you may be able to avoid something like sudden cardiac death to actually see a lifespan maximizing intervention in the future that has a high safety profile and a good amount of evidence.
3 Likes
These are perfect examples of “mice are not people”
Statins have such a great example of studies involving tens of thousands of cohorts that it would be foolish in my opinion to ignore the positive results of these studies.
Many studies involving large cohorts have found that statins can help to reduce the risk of heart attack and strokes.
1 Like
Agreed. Dr. Miller said as much.
It’s worth pointing out, and I’ve been stating all along, because something works in mice doesn’t mean it will work in humans. But the inverse is true also. There may well be some compounds that are ineffective in mice, but actually have benefits in people.
36:27 to 36:39 of Joe Cohen video.
As tongMD points out above, mice and chimps don’t get heart attacks. I am sure the scientists are aware of that. So I believe the simvastatin study was done for longevity not related to CVDs.
I only pointed to the available evidence. Whatever takeaway is an individual choice.
There is stated opinion here (rivasp12 I believe), that the longevity benefit of statins has to do with inflammation. So that may be why there is benefit in maximal lifespan of high-dose sim mice. What that high dose translates to, I have to poke around to calculate. But the takeaway for me is, if it is only reduction in inflammation that produces the longevity benefit, I can do that with other substances.
1 Like
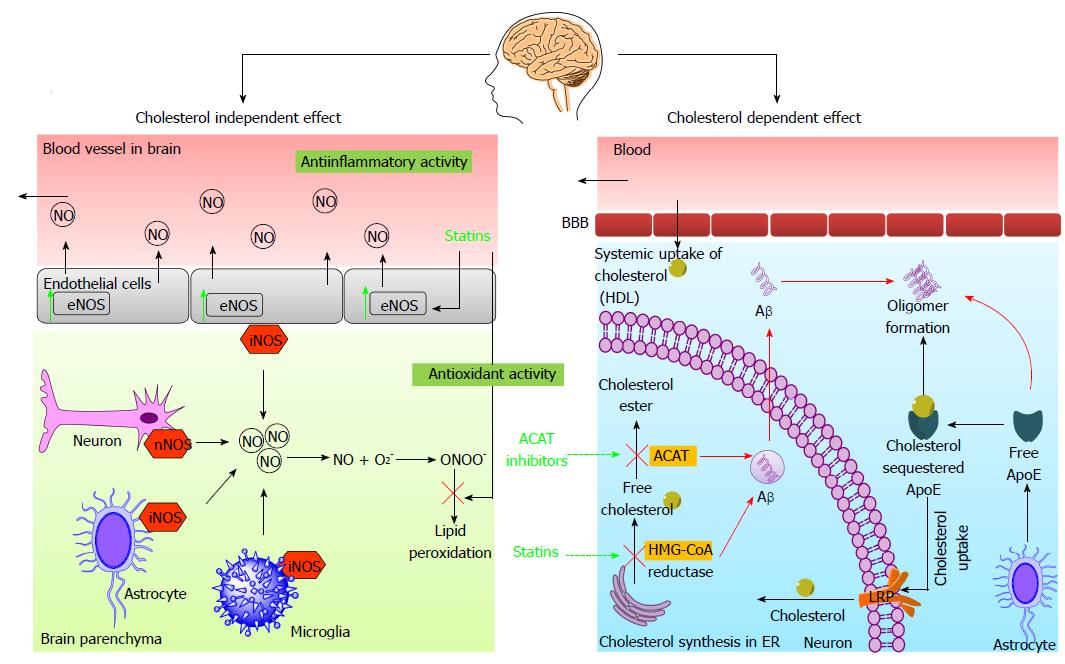
I’d also note, by the way, mice don’t get Alzheimer’s and some of the other neurodegenerative diseases we get. Alzheimer’s research towards preventive intervention is heavily underfunded and maximal lifespan probably doesn’t matter if one does not have intact cognition.
Alzheimer’s was an older white whale I gave up on in terms of the current types of interventions as opposed to biological aging but statins may be able to steer a neuron toward nonamyloid pathways due to the inhibition of HMG-CoAR - this suggests we get perhaps 2 pieces of the Alzheimer’s puzzle out of the way.
1 Like