We have a list of companies people here have used with success - List of Good Online Pharmacies
May I suggest you read the enclosure you got with your empagliflozin?
First, I don’t have type 2 diabetes, but I am old and my fasting glucose and A1c continue to slowly rise. My current fasting glucose level is 97mg/dL and A1/c is 5.5 % of total Hgb I have been on metformin for decades, first 500 mg daily and now 500mg twice daily. Metformin certainly has mixed reviews for someone my age. (81) So, I have been cycling on and off with other blood sugar-lowering supplements to see what effect they have on my fasting glucose. I take my blood glucose levels 2 to 3 times a day.
The blood sugar-lowering drugs and supplements I have or am taking are metformin, Jardience/Empaglifozin, berberine, and chromium supplements. I recently started trying Jardience/Empagliflozin tablets made by a German company Boehringer Ingelheim and imported to India by Boehringer Ingelheim India Private Limited.
Oddly, none of the things I have tried or am taking seem to have much of an effect on fasting glucose. Empagliflozin taken at 10 mg and 20 mg daily has had no discernible effect. Today I finally took out and read the Jardiance/Empaglifozin enclosed literature. I was surprised at the almost innumerable side effects they had listed from relatively large cohort studies ~70,000. They supply a surprising amount of information about the drug. Also, the benefit compared to placebo at various doses and with and without metformin was not very impressive.
So at this point, I am going to forego metformin and empagliflozin because for me the risk vs reward benefits aren’t there.
Bottom line: For me personally, metformin, empagliflozin, berberine, etc, has had little effect on my blood glucose levels. For younger people there may be longevity effects with the metformin.
i am 70 and not diabetic, currently taking canagliflozin 50 mg daily (cut 100 mg pill in half), and 25 mg acarbose on meal times. my fasting blood glucose drops from 108 in December 2021 to 88 in April this year. I also lost 10 pounds weight in between. IMO, the combo works better than metformin i took before.
1 Like
Good for you, though I personally found that losing weight alone lowers blood glucose.
Well, possibly in my case, you can’t fix what is not broken.
Interestingly while I was on a ketogenic diet I discovered that potassium BHB salts would dramatically drop my blood sugar in 30 minutes. People on a ketogenic diet tend to have a higher than normal fasting blood sugar level. BHB salts were recommended to help transition into ketosis. I use the potassium for two reasons, I like the blood pressure-lowering response to the potassium, and two, the potassium salt can be taken in a glass of water because it is not as nasty-tasting as the other BHB salts I have tried
1 Like
Thanks for the advice. I only take Empagliflozin(10mg) and Rapa(2mg), but with the SGLT2 inhibitor I take it occasionally and not daily(usually when I know I will be eating out or not the healthiest). I have not felt any side effects nor seen a drop in fasting glucose, although as far as I understand SGLT2 inhibitors just prevent the ability of glucose from being reabsorbed, so not sure if I would expect a significant drop in fasting glucose?
Thanks again though, have you had any side effects in your experience?
No, I had no side effects. I just stopped taking it because it didn’t seem to have any detectable effect on my fasting glucose levels. It may affect peak levels, but I didn’t measure that.
If it is doing you some good I wouldn’t stop taking it.
You know that the entire focus of sglt2 inhibitors is to blunt the peak glucose levels, and that is what is thought to be the mechanism for life extension in the NIA ITP studies.
Fasting glucose would not be impacted.
See here:
3 Likes
After reviewing many articles, I’m more bullish on SGLT-2 inhibitors than ever. They seem to proffer many cardiovascular and renal benefits, and some of these may be independent of its glucose lowering actions.
See:
https://www.nature.com/articles/s41569-020-0406-8
- The cardiovascular benefits manifest rapidly and are unlikely to be related to the improvement in glycaemic control.
- Early natriuresis, reductions in plasma volume, improved vascular resistance, reduced blood pressure and changes in tissue sodium handling might underlie the rapid reduction in the risk of heart failure.
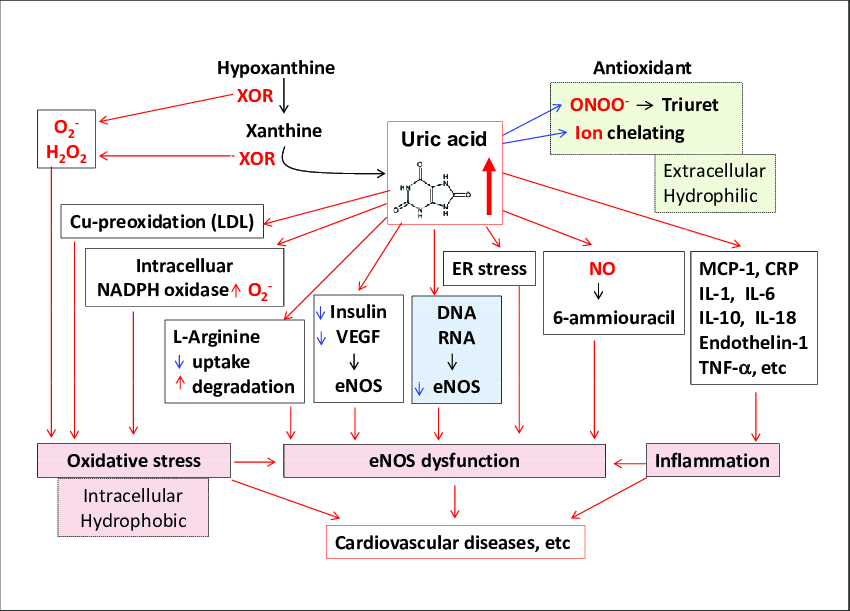
- A shift towards ketone body metabolism, reduced serum uric acid levels, reduced adipose tissue-mediated inflammation, decreased oxidative stress and suppression of damage mediated by advanced glycation end-products might also provide benefit.
https://journals.sagepub.com/doi/full/10.1177/1479164114559852
https://www.nature.com/articles/s41581-022-00535-6
SGLT2 inhibitors are consistent across many patient subgroups, including those with and without type 2 diabetes, at different stages of CKD, and in patients with heart failure with preserved or reduced ejection fraction.
This article talks about the synergestic effects of combining GLP-1 RAs with SGLT-2 inhibitors, where SGLT-2 inhibitors still do most of the heavy lifting.
3 Likes
That said, I still take it on an as needed basis, especially an hour or so before large / carby meals, and don’t take it much when I’m following a ketogenic diet or fasting.
1 Like
Thanks, I wasn’t really aware of the cardiovascular benefits for non-diabetics.
Since I have a year’s supply of Jardiance from Boehringer Ingelheim Pharmaceuticals guess I will start taking it again at a low dose. Most of the benefits cited are for type 2 diabetics.
One of the effects I overlooked until now is the lowering of uric acid levels.
This explains my sudden drop in uric acid levels from my last blood test.

“Empagliflozin was approved for medical use in the United States and in the European Union in 2014.[2][12][13][7] It is on the World Health Organization’s List of Essential Medicines.[14] In 2019, it was the 146th most commonly prescribed medication in the United States, with more than 4 million prescriptions”
“Developed by
Boehringer Ingelheim Pharmaceuticals and Eli Lilly and Company”
Empagliflozin - Wikipedia.
I have been on the anti-aging quest for decades.
While I am no Michael Lustgarten, I follow him on his Youtube channel “Conquer Aging Or Die Trying” Love his channel name, fits my goal exactly.
I am close to obtaining the goals that I set for myself and now I am just doing some tweaking from time to time. That is why I am here; to benefit from the knowledge and experience of others.
2 Likes
Do you think uric acid drop must have been mainly due to empagliflozin? Were you also taking quercetin in the meantime, for example? Q also reduces uric acid.
Slightly lower uric acid is not really a problem at least going by Rick Johnson’s work, and David Perlmutter also published a book recently with this thesis: Drop Acid: The Surprising New Science of Uric Acid - The Key to Losing Weight, Controlling Blood Sugar and Achieving Extraordinary Health - Kindle edition by Perlmutter, David. Health, Fitness & Dieting Kindle eBooks @ Amazon.com.
")
Dr. Stanfield pretty much deatroys Perlmutter’s uric acid hypotheses in the video above. I haven’t looked at the research myself, but he’s pretty convincing.
I have been taking quercetin for a very long time. Maybe it has some synergistic effect. I will keep an eye on it.
Thanks for the reference on uric acid.
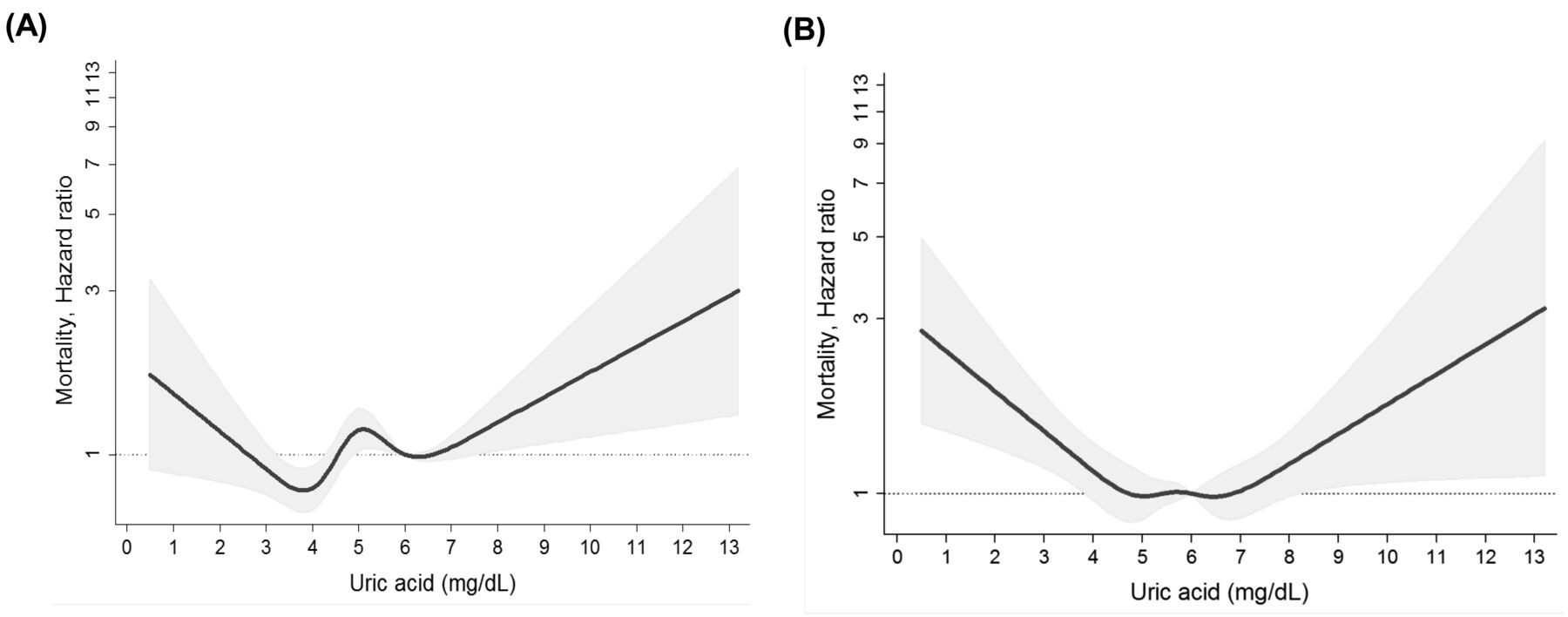
And then I found this: Significance of serum uric acid levels on the risk of all-cause and cardiovascular mortality - PubMed
This paper indicates that my uric acid level may be optimal, but it is a small study.
It appears that the optimal level of uric acid is still open for debate as there are many conflicting studies.
1 Like
Thanks for sharing this. Yeah I’m not sure how the dementia related hypothesis stands.
But it looks like Rick Johnson is onto something important with the role of fructose being harmful, with many of its effects also being driven by the production of uric acid, which has a role to play in kidney function, hypertension, etc.

1 Like
Perhaps no one is reading this thread, but what the hell…
I am 2 weeks into Empagliflozin 10 mg for 1 week, then up to 25 mg daily. I am not exactly lightheaded, but similar. I haven’t tested it, but I think this may be similar to what I have heard from athletes on a ketogenic diet. It feels like I have slightly less blood sugar, so if I get used to this new energy state, perhaps I will adapt to this. Of course, this is wildly subjective and speculative. I don’t have a BG monitor around. I am peeing more, and my end-of-the-day leg swelling seems reduced.
It was reading about renoprotective effects (I have forever had a slightly elevated creatinine) and the cardiovascular remodeling benefits that have been postulated.
https://pubmed.ncbi.nlm.nih.gov/35320057/
3 Likes
Dr. Stanfield did not present that problem well. Uric acid is not just an antioxidant it is a prooxidant. There are suggestive pro-oxidative effects of uric acid in CVD.
Hyperuricemia also may increase the risk of hypertension, CKD, and higher mortality of CHF. We know these factors may increase the overall risk of dementia and there is not enough to establish a causal line of evidence, although there are a few hints of it:
“Risk of dementia, especially vascular or mixed dementia, may be increased with high SUA levels in elderly people.”
It could also just be that it’s more a sign of dehydration. Also, normal uric acid doesn’t rule out gout. Some people can have concentrated uric acid to the point of saturation only in their extremities.
Unless one has a family history of gout and other risk factors (maybe <5.8 would be better), maybe I’d consider 5-6 being a possible target goal - but we don’t know for sure - may not matter in those ranges.
On the other hand, familial renal hypouricemia has an increased risk of AKI, and recurrent AKI which leads to CKD. So uric acid does have antioxidant capabilities that are important when too low.
2 Likes
If you’re particularly interested, there are manufacturer coupons for prescription CGM for free 2 weeks of use for convenient data collection. I’d probably shy away from too many anti-hyperglycemic medications (and occasionally certain foods) combined at once although I don’t generally think hypoglycemia would be a concern for even a two-drug combination of most of the drugs proposed here on their own.
I have elevated creatinine slightly higher than normal most likely from creatine monohydrate (Creapure) intake and higher than average lean mass. Every Cystatin C test for years has been completely fine but eGFR always looks horrible on older creatinine-based calculations. You may be interested in the newest equations here, just in case:
I did a Cystatin C recently in the high range of NL. My creatine is the way it is because I’m 6’ 6", 247 lb and it’s mostly muscle from sports; I also had a R quadriceps compartment syndrome in 2009, and the scar tissue continues likely to keep creatine high. I could be wrong, But my BMI is not a good way to assess my eGFR. But I was led to believe I had moderate CKD for the longest time. I don’t believe it anymore.
I had heard it was a myth that Micronized Creatine Monohydrate Capsules could increase creatinine, and I haven’t seen anything that disputes this, but I remain open-minded. Thanks for the suggestion of CGM.
1 Like
DrM, did you check your blood pressure? SGLT2 inhibitors have a mild osmotic diuretic effect which might explain your lightheadedness.