Any actionable advice we can takeaway from this paper?
3 Likes
I feel that the Threshold Theory of Senescence is closest to being the most reasonable way for humans to live with senescent cells.
That does require clearing excess cells above the threshold line or the eventual harm they cause will be beyond any control posed by “macronutrients” in a relatively healthy individual.
Since there is not yet a universal senolytic (except maybe FOX04-DRI) the senescence puzzle is far from being fully solved.
So I’ll keep doing 4 cycles a year of what I have available to me ![]()
2 Likes
I posted the same paper further up the thread with a bunch of findings that might be useful
2 Likes
Can you explain the details of the “4 cycles” you do Steve?
2 Likes
What is your baseline CRP?
I think that is the easiest way to measure teh senescent burden, but you need to do multiple measurements and take the lowest to exclude infection results.
1 Like
Basically the clinical evidence to date indicates that the “hit and run” timing or “cycles” as I call that process, is effective in managing aspects of senescent cell (SNC) “count”. I’ve posted links to those 2 important studies that demonstrates this.
Those 2 x Phase 1 studies showed that senolytics, when consumed by humans does clear SNC’s. The term “hit and run” was coined in these studies. High dose senolytics for a short period of time. That’s the fundamental of cycling, which any person who has used PED’s is familiar with, on and off the protocol for safety.
Since the body constantly creates senescent cells (BUT not a lot of them until later in life), and considering you don’t want to eliminate all of them (which is an impossibility) this cycling process allows for the “safe” removal of some senescent cells, in some parts of the body, but not all parts.
We have been doing 4 cycles a year since 2019. Our cycle is 3 days on and 4 days off for 4 consecutive weeks. Because we don’t use Dasatinib, our formula compensates for that. We also use the 2 polyphenols Quercetin and Fisetin at very high doses for those 3 days on. Added to that are some other compounds to increase bio-availability (polyphenol flavinoids are notorious for poor avalability) and a couple other things that are in it to improve it’s overall performance and digestibility.
Another important aspect of this whole senescent cell thing is the number of cell types in our body, about 240 types. Many of those types can become senescent. So there is not 1 senescent cell type and not 1 SASP profile and not 1 location and not 1 tissue type being affected. They can all be affected. Because of this, types, locations, etc. there is also not 1 senolytic (maybe one, but not commonly available) that can clear all types in all locations.
For example the Dasatinib + Quercetin protocol affects senescent cells in adipose and endothelial tissues. And it is weak on passing the blood brain barrier.
So the prevailing theory that is constantly being tested in all the trials I’ve read is “hit and run” or cycling…
6 Likes
According to this, the Mayo Clinic senolytics trials (D+Q and Fisetin) have been completed but results will be published in the next couple of years.

2 Likes
Received our FOXO4-DRI last week.
The dosing information on this one is worse than trying to sort out Rapamycin LoL!
3 Likes
What did you decide for dosing? I’m considering trying a few cycles but have no idea how much I will need to purchase.
I’ve seen dosing range from;
3x 25mg doses in 5 days - i.e. on-off-on-off-on then cycle again in 6 or 12 months
6x 3mg doses in 11 days
6x 1mg doses in 11 days
Each one of those cycles is 1 day on, 1 day off until the cycle is completed. And do that once or twice per year.
I’ve settled on the 6x 3mg (18mg total) in 11 days for my first experiment. Will be doing that in Jan as I’m finishing up our TA-1 experiment the end of December.
1 Like
Thanks for the prompt response. When 10mg is $300, I’m not sure if I can afford multiple cycles.
These results support the relevance of SASP proteins to human aging, identify specific traits that are potentially affected by SASP, and prioritize specific SASP proteins for their utility as biomarkers of human aging.
2 Likes
Senolytic therapy preserves blood-brain barrier integrity and promotes microglia homeostasis in a tauopathy model
https://www.sciencedirect.com/science/article/pii/S0969996124003127?via%3Dihub
3 Likes
IMO: The best senolytic therapy is rapamycin or the DAV protocol.
Try reading the DAV Therapy thread. Detailed information is given about the protocol.
“My DAV* Therapy Experiment begins! *Doxycycline, Azithromycin and Vitamin C”
The ingredients are available from India for a reasonable price, if you are able to receive exports from India.
The therapy uses Azithromycin + Doxycycline + Vitamin C.
"The present approach effectively eradicates senescent cells and cells carrying the hallmarks associated with aging.
I have tried the protocol twice. Did I notice any subjective effects? No…
These have been posted before:
6 Likes
Do you cycle between DAV and Rapa or favor one approach over the other?
1 Like
I have used both. Currently, I am on vacation from rapamycin. I plan on starting rapamycin again next year. I have tried the DAV protocol twice, and there are no subjective results.
I am unaware of any practical, affordable, available cell senescence tests, so you have to take a leap of faith when using these protocols to reduce cell senescence.
5 Likes
I feel like much of what we do is a leap of faith as the placebo effect is hard to objectify. But as most of us are already in very good or perfect health, it’s difficult to see many changes without specific and expensive testing.
5 Likes
Senescence is a 2 edged sword, some is beneficial but the nature of an “immortal” cells type that is hard to clear out, especially as the immune system declines causes significant increase in inflammatory response that no amount of “lifestyle” can fix.
2.4. Senescence-Associated Secretory Phenotype (SASP)
Cells may enter a senescent state as a consequence of various stressors, which further drives organismal aging. Cell cycle arrest is a typical feature of cellular aging; it leads to a stable, terminal proliferative halt and the development of a SASP [54]. The SASP defines the secretion of various cytokines, chemokines, growth factors, proteases, and lipids by senescent cells. This concept was first introduced by Krtolica et al. in 2001 [55]; they proposed that senescent cells secrete factors into their microenvironment, thereby potentially modulating biological activities both locally and systemically. In 2008, the SASP, also known as the senescence-messaging secretome, was independently characterized by various laboratories as primarily consisting of pro-inflammatory and growth-stimulating proteins [56,57]. This secretion leads to chronic inflammation and tissue damage in organisms. The composition of the secretome varies depending on the trigger of senescence, and the proportion of senescent cells in very old primates is estimated to range from 5 to 20% [58], contributing to age-related diseases. The SASP can also interact with immune cells, creating feedback loops that exacerbate tissue damage
[44].
Immune Alterations with Aging: Mechanisms and Intervention Strategies
4 Likes
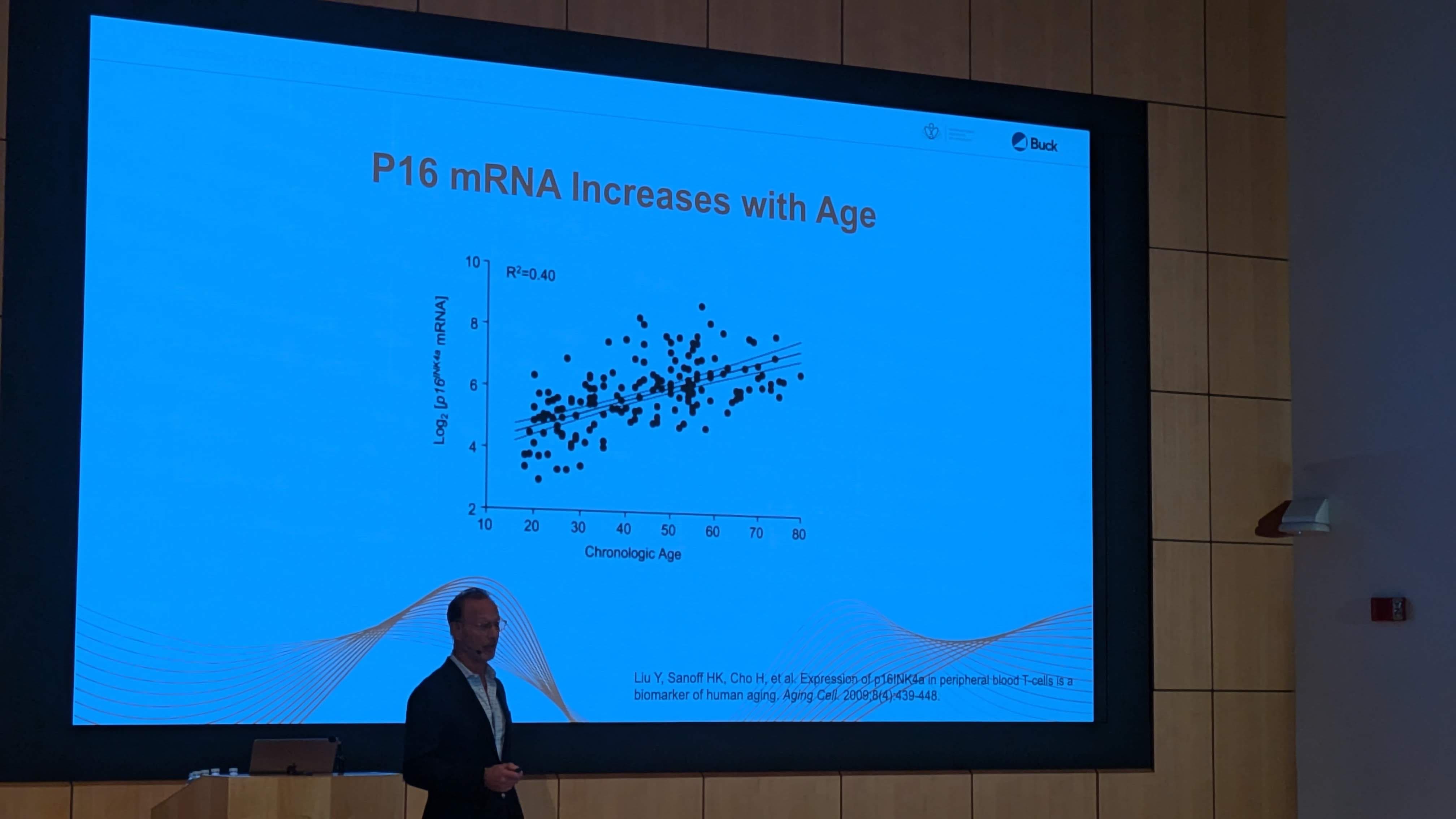
I’m going to do a full writeup on this - SapereX was at the conference this week and they have a test that I think retails for $650 for measuring P16 levels in the body. Its a test that is only starting to become available and only via certain longevity doctors (mostly in major cities) - so not available for most people, but it looks interesting.
More info on SapereX and the research they are based on: https://www.saperex.com/copy-of-early-access
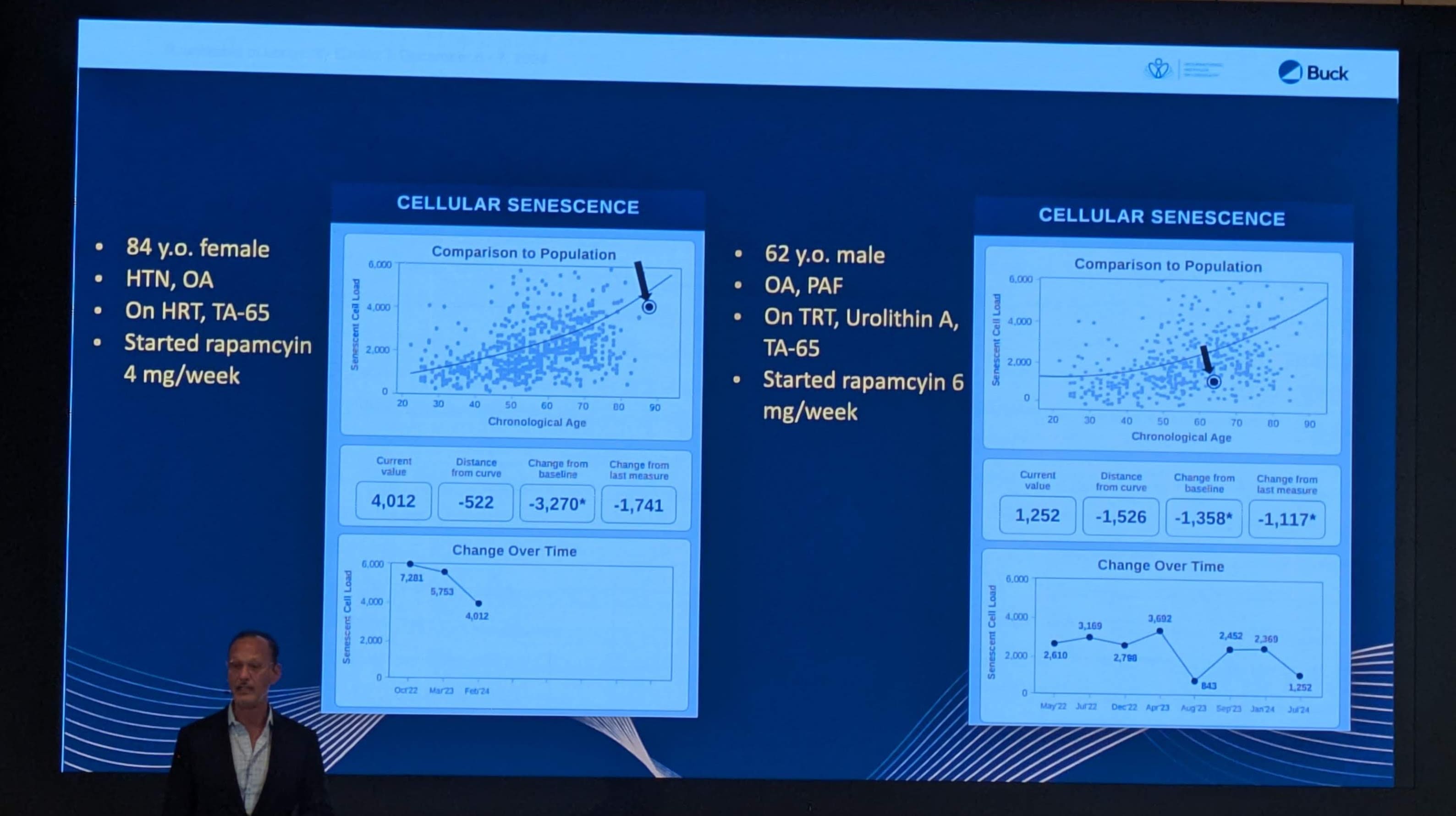
I’m doing a full report on this company/test in the near future with details, and we can discuss the pros and cons of this approach. I believe that this is the first commercially available scenescent cell load blood test that is becoming available, and doctors are using it as a metric to test to determine whether to prescribe senolytics (high dose fisetin and quercetin) and / or rapamycin.
and they are doing pre/post testing to show how these therapeutic approaches impact the senescent cell levels in the body:
7 Likes
This is an important test, hope it is as relevant as it appears to be.
@DrFraser will you have access to this test?
2 Likes