I found this paper on senescence which I thought I would share. Here are some key points:
Thus, the removal rate (as mice get old) falls by a factor of 5–20, and hence, senescent cell lifetime rises by the same factor. This is in reasonable agreement with direct measurements of lung Bleomycin-induced senescent cell removal in young and old mice [25], in which senescent cell half-life rose by a factor of about 5 (5 ± 1 days versus 25 ± 6 days).
This tells us that as mice age, senescent cells hang around creating inflammation 5X as long as when they are young. Probably similar for humans.
My hypothesis: If we assume that at middle age, the half-life is around 15 days, so a 2-week Rapamycin protocol may be more appropriate. Whereas when we reach old age, a 1-week Rapamycin protocol may be more appropriate as senescent cells cannot be cleared as quickly. Therefore, the younger you are, the longer you can go between dosing for maximum senescence prevention.
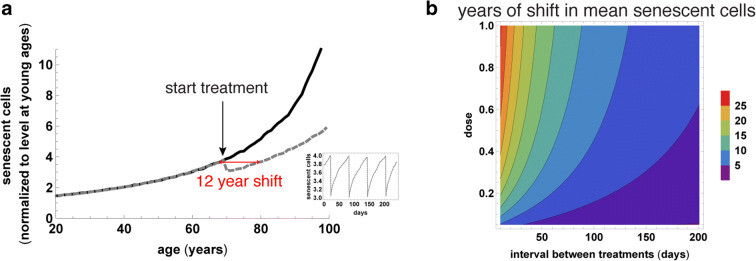
We therefore use the SR model with parameters calibrated for humans in Ref [25] to simulate senescent cell removal therapy with different temporal spacing between treatments. We find that treatment can be as infrequent as once per 2 months in order to maintain average senescent cell levels that are about 2-fold lower than without therapy (Fig. 6a, b). This amounts to a shift to senescent cell levels typical of a person 12 years younger. Thus, intermittent treatment with senolytics or immune therapy starting at old age and given once every 2 months may be a reasonable approach in humans.
This image gives you an idea of senescent cell loads in humans.
Based on these graphics, I would start a 60-day senolytic treatment at age 60. I believe the best senolytic right now is Dasatanib + Quercetin. Hopefully, there’ll be better treatments when I reach 60.
Rapamycin and Taurine should also prevent the senescent cell load from being as high as in the chart.
Just something to think about.
Full Paper: