It is. Do some queries on cortisol and / or glucocorticoids and ASCVD and you’ll get lots of hits…
Cortisol and cardiometabolic disease: a target for advancing health equity
Highlights
Stress in both intrinsic psychosocial and extrinsic physical environmental forms can impact the development of, and outcomes in, cardiovascular disease (CVD).
While experiences of or exposure to stressors may be acute or chronic, its severity and one’s ability to buffer against it is what may be most impactful on the body.
‘Toxic stress’ may affect the body through mechanisms involving the hypothalamic–pituitary–adrenal axis (e.g., cortisol).
Deviations in cortisol diurnal profile have been associated with adiposity, dyslipidemia, incident diabetes, and CVD such as hypertension.
Cortisol and its respective receptor, the glucocorticoid receptor, are involved in metabolism within adipocytes that may contribute to dysglycemia and insulin resistance and, therefore, cardiometabolic disease risk.
Glucocorticoid receptor antagonists and antagonists of the enzymes associated with cortisol metabolism may be promising targets for future research.
Acknowledging and addressing the contribution of stress physiology and cortisol in interventions to treat cardiometabolic disease at the individual, community, and population level are necessary to combat cardiometabolic disease.
Every living human develops senescent cells. However, as you get older, your body (immune system) gets slower and slower at removing them. While a given senescent cell may hang around for 2 or so days in a 20-year-old before being removed, that same cell will take around 20 days to remove for a 60±year-old. As you age, you have more senescent cells because your body can’t remove them as quickly or efficiently as when you were young. Hence the reason for starting senolytics at age 60+ And those senescent cells that hang around may also release SASP causing other normal cells to become senescent.
The solution is senomorphics such as Rapamycin, Taurine and Metformin to prevent senescent cell formation as well as senolytics at a later age (60+) to get rid of any that are hanging around.
Of course, older people develop more senescent cells. Since they aren’t cleaned up as quickly they propagate due to SASP. Therefore more senescent cells develop in older individuals. I’m sure there are other ways as well. This is just one example.
I don’t think either of us have any evidence as to whether the clear up percentage for younger people is higher or lower than older people. If you do I would be interested in reading it.
Which is the one referred to makes the assumption that senescent cells only disappear as a result of the immune system operating on them to kill them. We know that they can also stop being senescent and start functioning. (through senomorphic interventions)
Hence the assumption they base their paper on does not hold.
I think it holds for the majority of people who do not use senomorphics. Of course once you start using senomorphics, the game changes. However I still believe that senomorphics only slow down the accumulation of senescent cells.
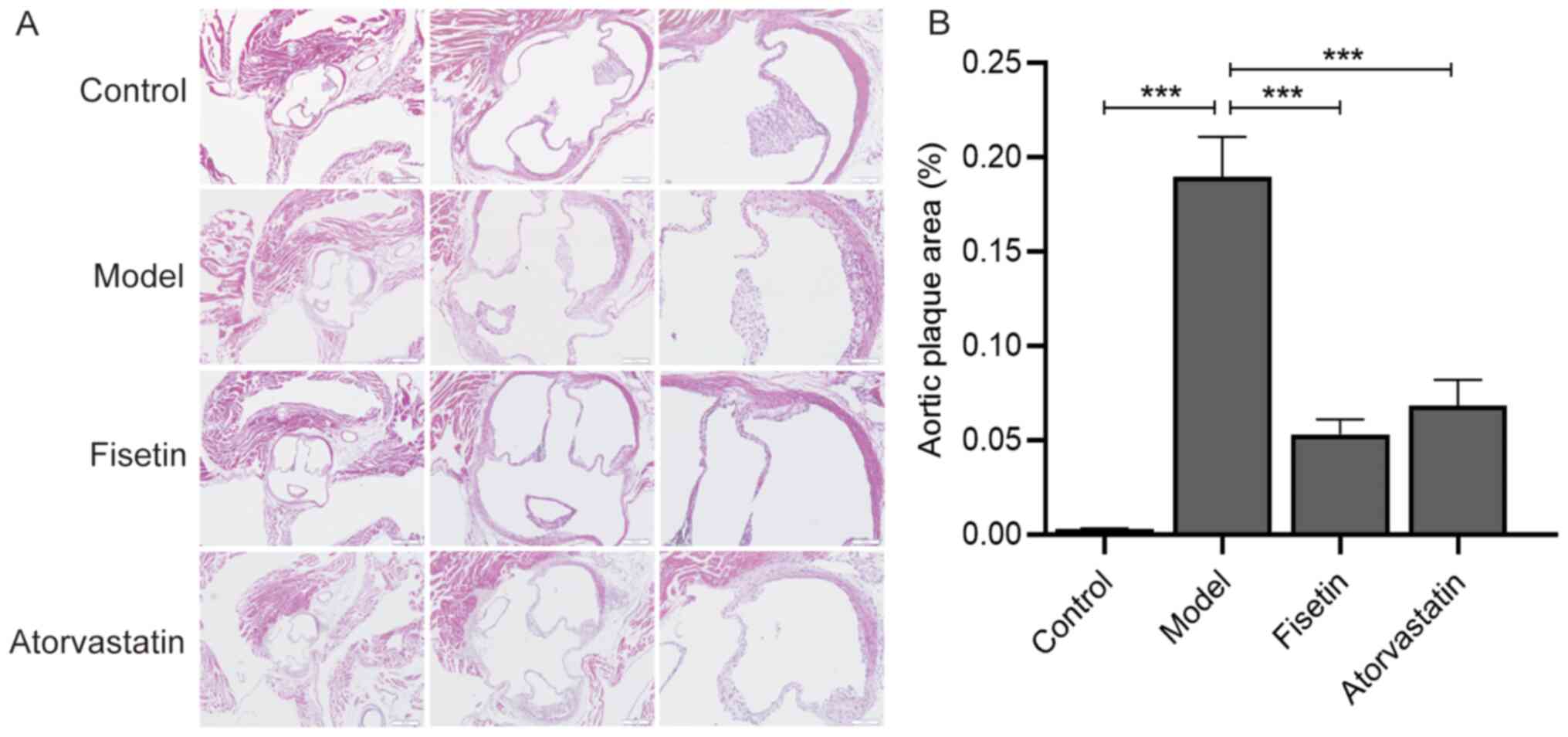
54 apoE-/- 12-week-old mice were fed a normal diet for 1 week before being randomly divided into three groups: apoE-/- mice + high-fat diet (model group; n=18), apoE-/- mice + high-fat diet + fisetin (fisetin group; n=18) and the apoE-/- mice + high-fat diet + atorvastatin (atorvastatin group; n=18).
Mice in the fisetin and atorvastatin groups were gavaged with aqueous solutions of fisetin and atorvastatin, respectively. Via conversion with reference to an adult body weight of 60 kg and the equivalent dose of mice, the final doses of fisetin and atorvastatin aqueous solutions provided to mice were 12.5 and 2 mg/kg, respectively. The fisetin was dissolved in 0.1% DMSO aqueous solution, and the atorvastatin tablets as a positive control drug were directly dissolved in distilled water. The control and model groups were treated with the same volume (0.2 ml/mouse/day) of distilled water via daily oral gavage, and the intervention period of each group was 12 weeks.
Combined with the results of previous in vitro experiments, these results suggested that fisetin may serve an atheroprotective role, ameliorating abnormal lipid metabolism by regulating the expression of PCSK9 and LOX-1, and improving senescence by regulating the expressions of p53, p21 and p16 (Fig. 5).
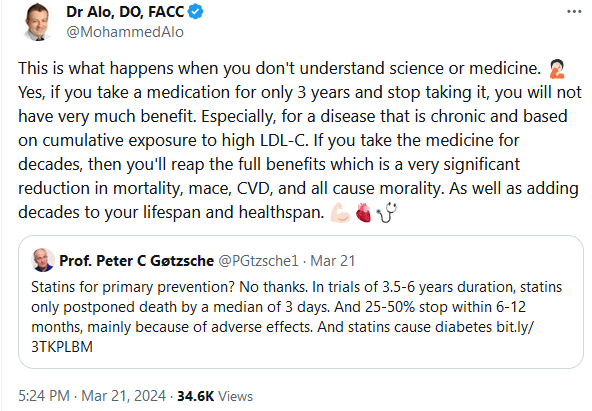
Dr. Alo seem like he is worth a follow. He explains the mistaken thinking some people have regarding statins. If the PREVENTABLE or STAREE study detect a positive effect on dementia, will everything change? Even if not, it doesn’t prevent someone from taking other drugs or therapies now.