This is not crazy. I shared a post by Mike Eades a while back about low carb diets reducing the lp(a). This has been known for some time.
From the article:
This is not crazy. I shared a post by Mike Eades a while back about low carb diets reducing the lp(a). This has been known for some time.
From the article:
This is a link to some interesting LP(a) articles Thomas Dayspring shared on X;
Table of Contents page: Atherosclerosis (atherosclerosis-journal.com)
If we accept it at face value, increasing Lp(a) while at the same time increasing apoB isn’t a good idea. I don’t know what that study is. Low carb diets iirc is associated with increased all cause mortality.
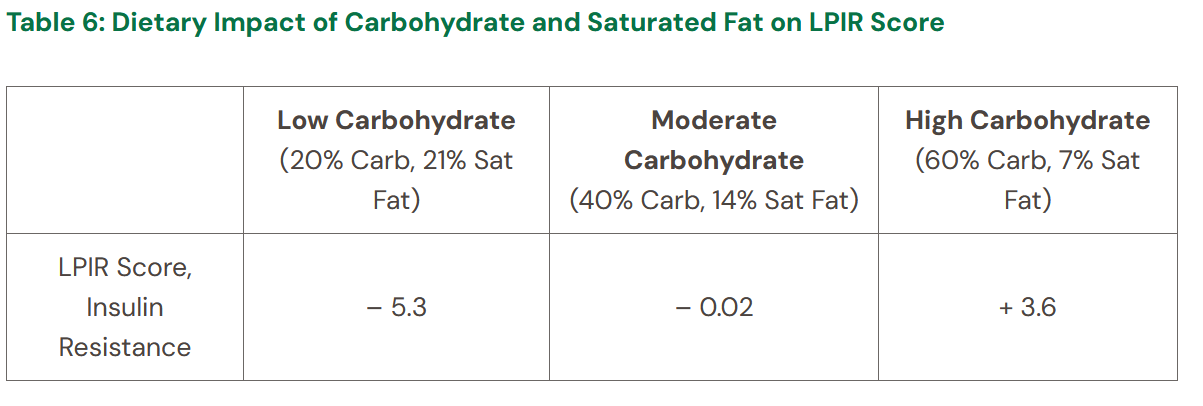
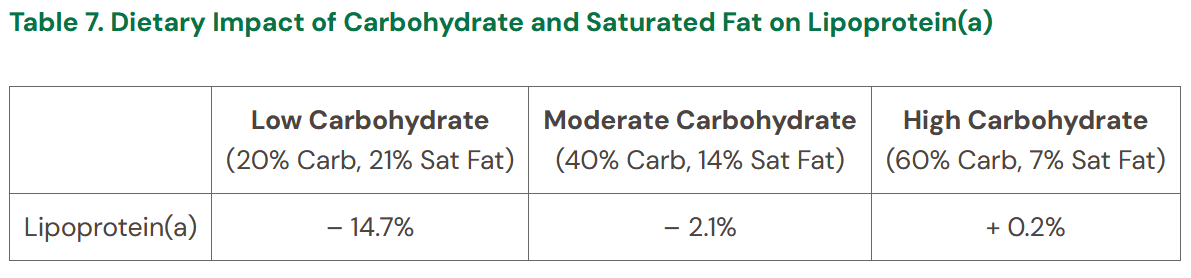
Not sure what data you’re looking at. Low carb diet with 21% sat fat reduces lp(a) by almost 15% according to this. Also according to this LPIR score is reduced by 5.3 and it is much more important than apob. They used a diet 20% protein and isocaloric, so as the carbs went down they increased the sat fat.
Also this table:
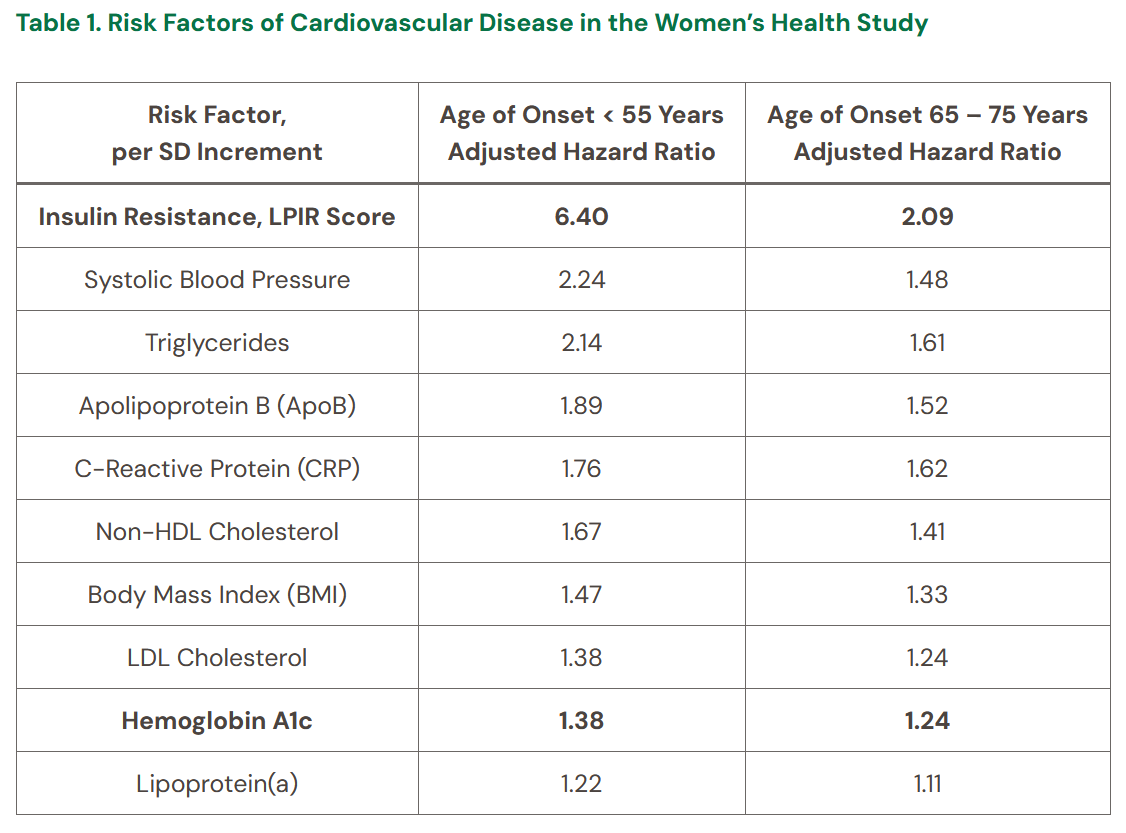
says LPIR is 5.5 times more important than lp(a) and 3.38 times more important than apob.
According to what study? It is a table. Please don’t post graphs to studies you have not read unless you say so explicitly. That at least shows you are interested in the truth.
I have responded to this here:
This is a quote from the article:
“In 2021, researchers from Mayo Clinic and Harvard Medical School published results from the Women’s Health Study investigating more than 50 risk factors and the incidence of cardiovascular disease at various ages of life.1 Specifically, this was a prospective cohort study of more than 28,000 US female health professionals, with follow-up spanning an average of 21.4 years. Participants did not have a known diagnosis of cardiovascular disease at the time of study enrollment.”
So the Mayo Clinic and Harvard were studying 28000 healthy women with a follow up of 21.4 years. This does not seem like nothing to me.
Is that table from the same study I already responded to?
Are you reading what I said or are you just ignoring it because that Mayo Clinic or Harvard did the study is not a response to what I brought up.
Click on the link to read the response.
I just reviewed all the relevant posts that precede this and that you linked to. I fail to see your point. If you carefully read the article…
https://kevinforeymd.com/insulin-resistance/
as I just did, it makes perfect sense and I can’t find a flaw. From the other thread, you say " LPIR is just a fancy way of measuring apoB and TG:" I think that the article above makes a very convincing case that LPIR gives early warning before changes in ApoB and TG and is therefor very valuable.
The problem is that those with high LPIR score has a lot of confounding factors. The study did not adjust for them. Once you start adjusting for them the LPIR decreases.
Because LPIR is basically just apoB and TG, if you adjust for that it will go away.
For example, if you combine apoB and TG into a measurement let’s say is called apTG, that will be more harmful than just apoB. Those who have high apoB and high TG are probably those with metabolic syndrome, etc, and be harmful in of itself. Of course it will have higher risk than apoB alone.
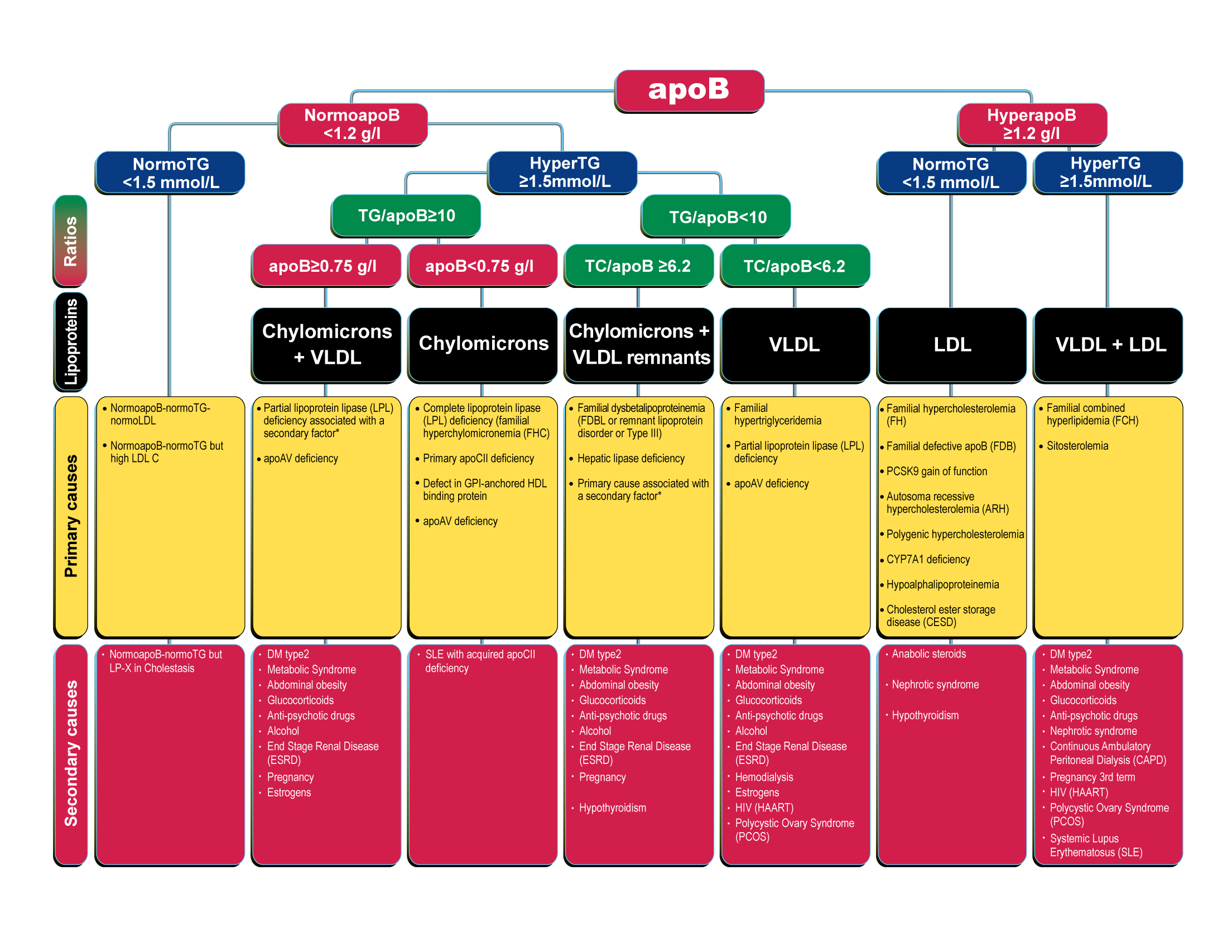
They had hyper apoB at 1.2 g/L and hyper triglycerides at 2 g/L.
Yes you will be at higher risk if you have high lipids AND are insulin resistant (high triglycerides - metabolic syndrome). That’s what the LPIR measures. It is not in exclusion of it, which people will be fooled into thinking (as it is not adjusted).
If you look at the women who get premature CHD before age 55, what markers would you see? Would it not be high apoB and high triglycerides, etc? Would they not be insulin resistant and have high triglycerides?
Would they only have high apob (but not astronomical)? No.
But I guess the people who have high apoB can make sure so they aren’t insulin resistant, that way they don’t have ultra high risk… Have fun with that house of mirrors.
Interesting paper. EPA/IPE reduces risk?
“Baseline Lp(a) concentration was prognostic for MACE among participants with elevated triglyceride levels receiving statin therapy. Importantly, IPE consistently reduced MACE across a range of Lp(a) levels, including among those with clinically relevant elevations.”
https://www.jacc.org/doi/10.1016/j.jacc.2024.02.016
https://x.com/Lpa_Doc/status/1773021487244701809?s=20
The point made in the article is that you would see a higher LP-IR score before you would see elevated ApoB and triglycerides and that is exactly why it is useful. It allows you to take action sooner. Are you discounting that?
I just did a very careful read through of this article on MR:
https://www.atherosclerosis-journal.com/article/S0021-9150(22)00192-7/fulltext
Then I came across this on Reddit: from Ricoss
"Have a read here where I explain what the lipids are used for. That should be the minimal understanding for anyone.
At a basic level, it will show you how insulin resistance is driven and how that reflects on your lipid profile. It will also show, theoretically at least, under what conditions atherosclerosis can be reversed.
Apart from that, the latest picture for risk assessment finds a very good correlation with lipoprotein insulin resistance (LPIR):
From approximately 50 biomarkers, lipoprotein insulin resistance had the highest standardized aHR: 6.40 (95% CI, 3.14-13.06) for CHD onset in women younger than 55 years, attenuating with age.
That is a quite high HR. Far from the usually very weak <2 in epi studies.
“Association of Lipid, Inflammatory, and Metabolic Biomarkers With Age at Onset for Incident Coronary Heart Disease in Women”
https://pubmed.ncbi.nlm.nih.gov/33471027/
In the next document, table 3 shows how the LPIR scoring is done.
https://www.liebertpub.com/doi/pdf/10.1089/met.2014.0050
You are supposed to score as low as possible.
Notice how it doesn’t say anything about total quantity of LDL.
Although from 2000, a good article to read on insulin resistance and dyslipidemia: Insulin resistance and cardiovascular disease - PMC
In essence, atherosclerosis, in general is a problem of insulin resistance. Endothelial cells are among one of the first to become insulin resistant and from that angle are responsible for a number of chronic diseases and symptoms. Seed oils (omega-6 PUFA) leads to a quicker insulin resistance."
That is not LPIR but Lp(a).
True…just wanted to preempt your “MR” strike.
Where did they say that and what is their source?
Did you even read the article?
Let me just give you somes quotes…then you can go and actually read the article.
“Meanwhile, emerging evidence suggests that insulin resistance is a stronger risk factor for the development of cardiovascular disease than elevated levels of LDL, ApoB, blood pressure, and obesity.1 In fact, insulin resistance appears to be a significantly more influential risk factor in the development of atherosclerosis than the traditional risk factors previously mentioned. This includes premature cardiovascular disease in adults less than 55 years of age, as well as cardiovascular disease at all ages.Therefore, some individuals with early stages of insulin resistance can still maintain normal blood glucose control, and thus, a normal HbA1c.The earliest manifestations of insulin resistance are characterized by elevated levels of insulin (hyperinsulinemia), which is a compensatory mechanism that allows the body to maintain normal levels of blood glucose during early stages of insulin resistance.In later stages of insulin resistance, blood glucose dysregulation can occur, resulting in abnormalities of HbA1c, continuous glucose monitoring, and fasting blood glucose. In summary, these traditional measurements of insulin resistance are effective at identifying later stages of insulin resistance, but often miss early stage insulin resistance.”
“Specifically, the LPIR Score has a unique ability to identify very early stages of insulin resistance, including those with normal blood glucose, normal HbA1c, and those with a normal body weight.”
“Importantly, the LPIR Score quantifies insulin resistance through a distinct biochemical pathway than that of Hemoglobin A1c and HOMA-IR, for which LPIR is particularly sophisticated in its ability to detect insulin resistance among those with a normal body weight and/or normal fasting blood glucose.”
“Specifically, the LPIR Score represented a stronger predictive risk of cardiovascular disease than all other measurements of lipoproteins, inflammation, blood pressure, and body mass index, per standard deviation increment.”
“Meanwhile, abnormalities in lipoprotein metabolism are observed many years before the onset of blood glucose dysregulation (hyperglycemia).”
If you don’t want to quote and source from the article specifically what you said that is fine with me:
I just want to find the source for this claim. The article can’t be trusted obviously, it is a blog post of a doctor who is not a cardiologist.
Alright…let me pull up some more studies. Is it the earliest predictor of heart disease? Well, Lp(a) is genetic, so if you’re asking - “Does it predict heart disease before conception?”…I think it does…but let me look for proof.
I can predict your point of attack…since the range of ApoB starts at 20, then 21 could be elevated ApoB.
Here is the study (since you don’t like the article). But the quote is the same…
“From approximately 50 biomarkers, lipoprotein insulin resistance had the highest standardized aHR: 6.40 (95% CI, 3.14-13.06) for CHD onset in women younger than 55 years, attenuating with age. In comparison, weaker but significant associations with CHD in women younger than 55 years were noted (per SD increment) for low-density lipoprotein cholesterol (aHR, 1.38; 95% CI, 1.10-1.74), non–high-density lipoprotein cholesterol (aHR, 1.67; 95% CI, 1.36-2.04), apolipoprotein B (aHR, 1.89; 95% CI, 1.52-2.35), triglycerides (aHR, 2.14; 95% CI, 1.72-2.67), and inflammatory biomarkers (1.2- to 1.8-fold)—all attenuating with age.”
You can’t multiply different hazard ratios like this.
It’s interesting because it’s clearly wrong.
A bit amusing to look at people come to the wrong and deadly conclusions because they are using one of the worst evidence available. They must come to their conclusions based on 62 women who got early CHD around age 48, who had high lipids, triglycerides, were obese, and in an association study.
Just like they come to conclusions based on the vaccine because of dozens of reports or anecdotes.
It’s almost as if bad scientific thinking is nothing strange to them because they have severe bias. They like to accuse scientists of bias, when in reality they are just projecting.
Lp(a) is six times more atherogenic than apoB:
Not like the table says “Lp(a) 1.22” “ApoB 1.89”.
I have already responded to this multiple times.
I am not going to repeat what I already said.
It is also hijacking a very good topic about Lp(a) to discuss this over and over.