G’day fellow Rapamycin News forum members
I hope this post finds you all in good health! Today, I come to you with a specific concern regarding my recent blood test results, which showed a high level of LP(a). I wanted to reach out to our community, especially those who have experienced similar situations or possess medical expertise, to seek advice and gather insights.
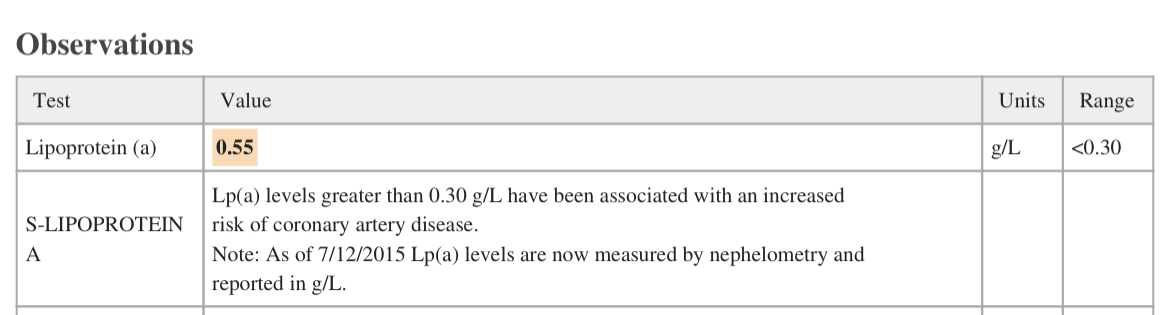
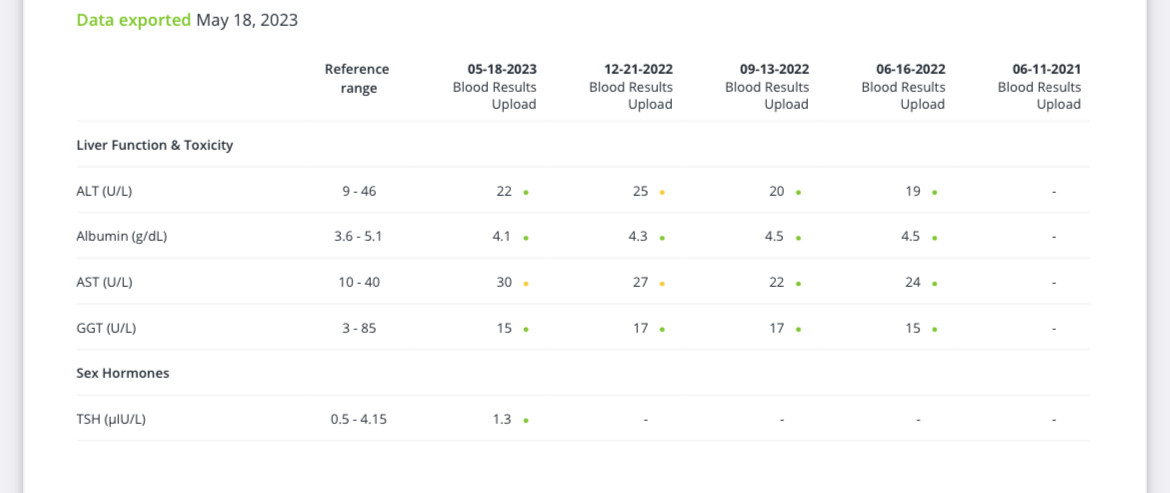
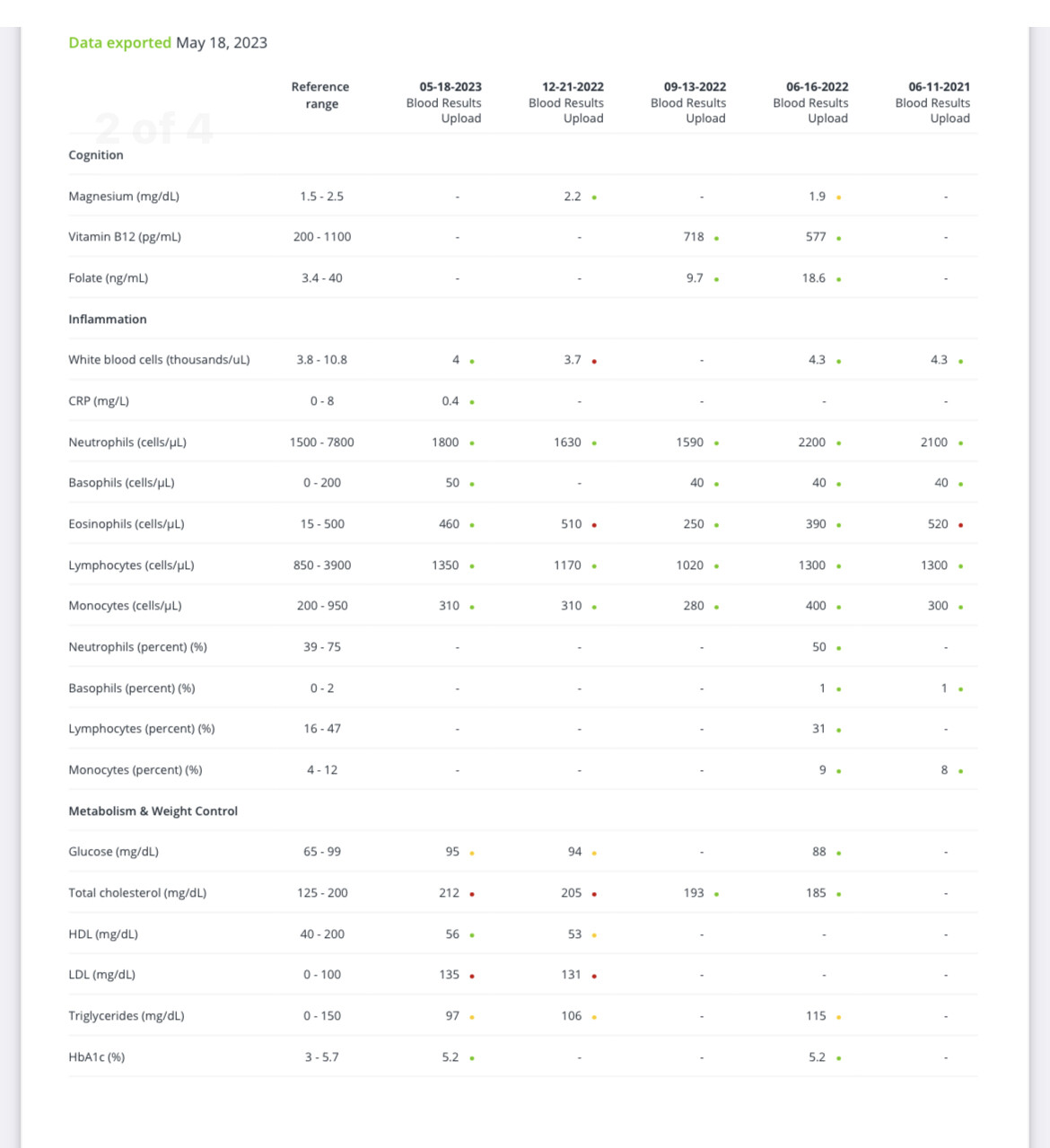
To provide some background, I am a 44-year-old male who generally maintains a healthy lifestyle. I exercise regularly, follow a nutritious diet, and consume alcohol moderately. Have posted my bloods below (elevated levels of AST, LDL, and glucose). CAC score of 0 and echocardiogram showing no evidence of stenosis. However, in my latest test, my LP(a) was measured and I’ve hit the genetic jackpot as it stands at 0.55g/L (screenshot below).
My main query is directed toward those who have faced a similar situation in the past. I would greatly appreciate it if you could share your experiences and let me know what advice your doctor provided. Understanding how others have managed or addressed high LP(a) levels would be incredibly valuable to me.
Additionally, I would love to hear from those who are knowledgeable about LP(a) or medical professionals among us. Are there any specific treatments or interventions you would recommend for high LP(a) levels? I have already come across PCSK9 inhibitors during my research (Attia’s Outlive book and podcast no 210) but I am curious if there are other approaches or treatments that have shown promising results (aware of niacin - seems to be some debate around the effectiveness of this?).
Now, turning the conversation towards Rapamycin, I currently take this and want to continue doing so. I am interested to know if any forum members who have high LP(a) levels informed your doctor about this? Was thinking about paying the GP to read the Evaluation of off‐label rapamycin use to promote healthspan in 333 adults paper…….
Lastly, I would like to mention that my long-time doctor has relocated (while they didn’t prescribe me Rapa, they were aware that I was taking this off label). So essentially this means I will be seeing a new GP. As a result, I am faced with the challenge of establishing a new doctor-patient relationship along with the above.
Thank you in advance for any advice you might give me.
Cheers
Dan