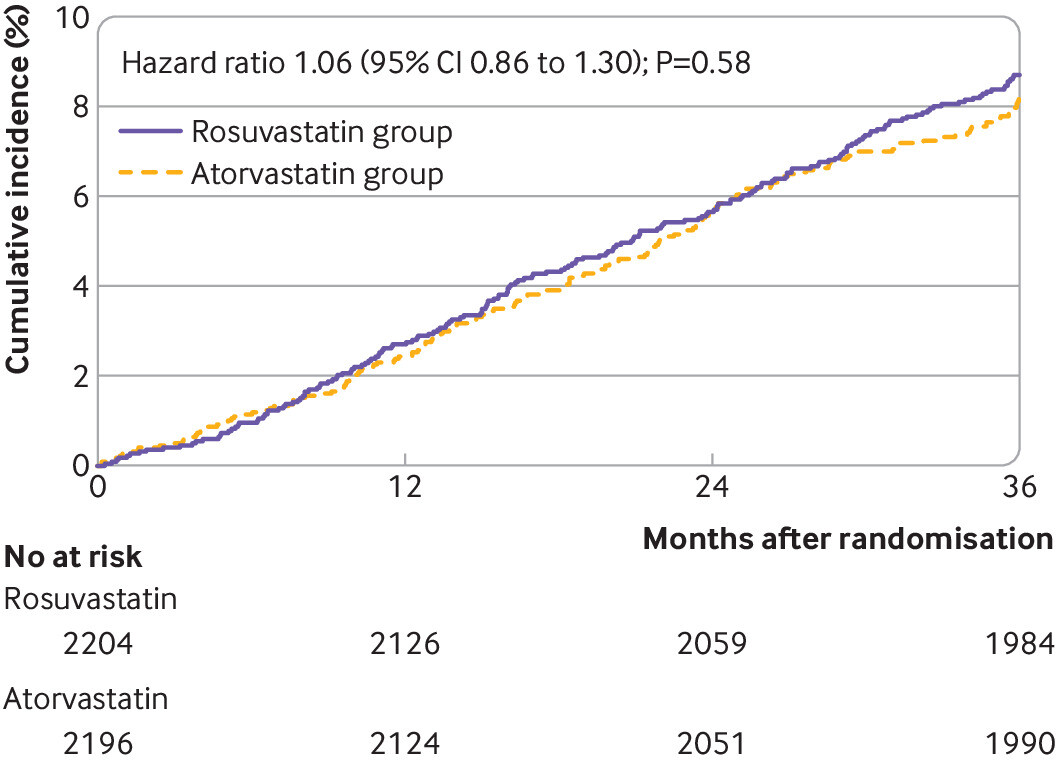
Results 4341 of the 4400 participants (98.7%) completed the trial. Mean daily dose of study drugs was 17.1 mg (standard deviation (SD) 5.2 mg) in the rosuvastatin group and 36.0 (12.8) mg in the atorvastatin group at three years (P<0.001). The primary outcome occurred in 189 participants (8.7%) in the rosuvastatin group and 178 (8.2%) in the atorvastatin group (hazard ratio 1.06, 95% confidence interval 0.86 to 1.30; P=0.58). The mean low density lipoprotein (LDL) cholesterol level during treatment was 1.8 mmol/L (SD 0.5 mmol/L) in the rosuvastatin group and 1.9 (0.5) mmol/L in the atorvastatin group (P<0.001). The rosuvastatin group had a higher incidence of new onset diabetes mellitus requiring initiation of antidiabetics (7.2% v 5.3%; hazard ratio 1.39, 95% confidence interval 1.03 to 1.87; P=0.03) and cataract surgery (2.5% v 1.5%; 1.66, 1.07 to 2.58; P=0.02). Other safety endpoints did not differ between the two groups.
If you are using rosuvastatin, would you switch to atorvastatin? What do you think of this study?
Whereas lipophilic statins such as atorvastatin can cross cellular membranes through passive diffusion and are therefore widely distributed in different tissues, hydrophilic statins such as rosuvastatin are more liver selective owing to the active carrier mediated uptake mechanism, and thus they are more limited in their ability to have additional effects beyond cholesterol lowering (pleiotropic effects) in extrahepatic tissues
That rosuvastatin is hydrophilic and more hepatoselective could be useful to not decrease brain desmosterol levels for apoE4 carriers.
I have been taking 40 mg daily for decades with no ill effects that I am aware of.
Two arguments for atorvastatin.
I. I tried some other statins and atorvastatin was the one that produced the least amount of side effects. (I have not tried rosuvastatin.)
2. Atorvastatin is one of the most studied drugs in history, with literally many 10’s of thousands of people studied.
Atorvastatin may not be the best statin, but it is the most studied and I know what I am getting.
The mean daily dosage was 36 mg for atorvastatin and 17.1 mg for rosuvastatin, meaning most were at 40 mg or 20 mg, respectively. It is promising that it showed fewer side effects in this study compared to rosuvastatin.
At first glance it does appear that atorvastatin is the somewhat safer drug. If one is at risk of diabetes and can tolerate either statin, perhaps using atorvastatin might be the better alternative.
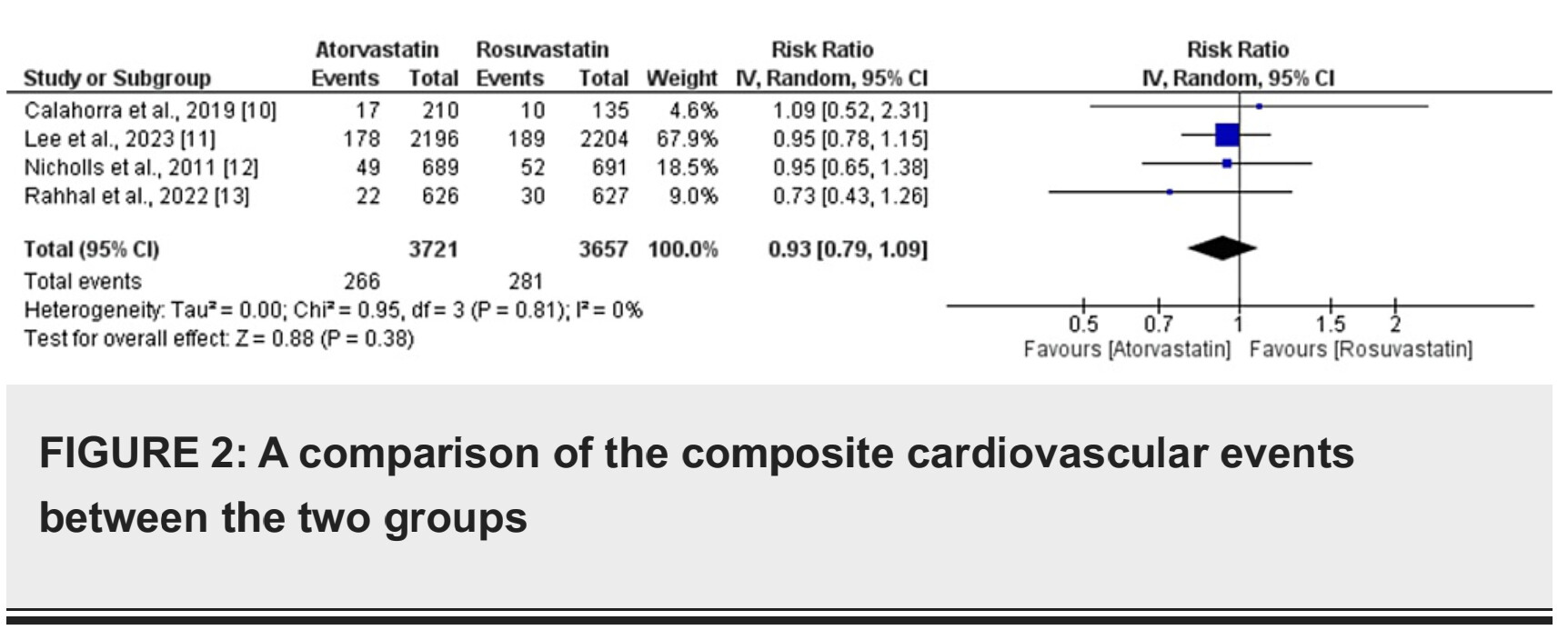
Atorvastatin seems a bit better (although not statistically significant) in terms of “three year composite of all cause death, myocardial infarction, stroke, or any coronary revascularisation”. But what about all-cause death only?
It should be available open access at the link. No statistical difference for all-cause death.
P-value at 0.38 does seem a bit noisy, almost 40% chance result could be due to chance.
Thanks it’s so weird I couldn’t see the full text on desktop but I can read it on mobile…
Anyway: If you believe the findings of the Jupiter trial regarding ACM why don’t you believe this trial?
All cause death occurred in 57 participants (2.6%) in the rosuvastatin group and 51 (2.3%) in the atorvastatin group (1.12, 0.77 to 1.63; P=0.57)
We can very safely say based on this trial (+ others in the meta analysis) that atorvastatin is not inferior to rosuvastatin when it comes to ACM. So IF rosuvastatin reduces ACM compared to placebo then atorvastatin does the same.
But then, looking at the data, and although it’s not statistically significant, it seems that atorvastatin might be a bit better than rosuvastatin in terms of both ACM and primary composite outcome.
So, for someone starting a statin, atorvastatin seems the best choice as of today. No?
The reduction in ACM in JUPITER was statistically significant, at P=0.02.
If a trial existed for atorvastatin that detected a decrease in ACM it would become more interesting to me. I don’t know if one exists.
If there are two drugs, of which one has detected a decrease in ACM in a clinical trial, I should choose that one over others, no? (As it is related to net benefit).
I wrote elsewhere also this:
I chose rosuvastatin over atorvastatin:
I already had success with rosuvastatin.
It is not metabolized at CYP3A4 which mean I can try rapamycin later with GFJ, and also fewer drug interactions I guess.
It being hydrophilic might give benefits.
I can monitor diabetes risk anyway so it doesn’t matter that much that is has a higher causal risk compared to atorvastatin.
Trial 2 says that drug X and drug Y are equivalent in terms of ACM.
Conclusion: drug Y also reduces ACM vs placebo.
It’s just transitivity of the relation of inequality: if X < P and Y = X then Y < P.
Here trial 1 = JUPITER. Drug X = rosuvastatin. Trial 2 = LODESTAR. Drug Y = atorvastatin.
In this particular case, it’s even better because not only LODESTAR showed “comparable efficacy” but it also signaled a potential (but non statistically significant) superiority of atorvastatin vs rosuvastatin.
Because that’s the conclusion of the authors of the trial.
One more thing: in Table 2, they looked at 15 individual outcomes (actually a bit more if you include sub outcomes but it’s the same reasoning and it would make the case for atorvastatin even stronger so let’s exclude them). Out of these 15 outcomes, atorvastatin is superior to rosuvastatin in all but one: Peripheral artery revascularisation (0.5 VS 0.8, not statistically significant). Most of these differences are not statistically significant (cataract surgery and new onset of T2D are though). However, if the differences between atorvastatin and rosuvastatin were entirely due to chance then we would have about half of the outcomes for which rosuvastatin outperforms and the other half showing superiority for atorvastatin. Not 93% for atorvastatin (14/15) and 7% for rosuvastatin (1/15).
It is possible, but I would not say that atorvastatin reduces ACM because there is no statistical difference in a comparison between atorvastatin and rosuvastatin. In fact, there should be no difference between any statins (no power). That doesn’t mean they are all equally good when it comes to ACM. You can also do a heads on comparison of different classes of drugs, like Crestor vs. PCSK9i, or ezetimibe, conclude no difference. Does not mean that PCSK9i decreases ACM or ezetimibe, I think that has to be established in a clinical trial vs. placebo.
The estimated HR for drug Y compared to placebo is approximately 0.714, suggesting a 28.6% reduction in the hazard of outcome 1 compared to placebo. The 95% confidence interval for this indirect comparison is 0.47 to 1.09.
It’s important to note that this estimation and its CI are based on indirect comparisons and carry the assumptions and limitations associated with such methods. Ideally, these results should be confirmed with direct comparative studies.
So it became wider and statistically insignificant.
I would like to know why JUPITER detected ACM benefit, while atorvastatin trials doesn’t seem to. What the explanation for that is. It would require a lot of research. (Might it do with the high CRP in JUPITER?).
I like the heuristic of prioritizing drugs with ACM benefit vs. placebo.
One of the other areas I look at is the controversy on hydrophilic vs. lipophilic is neurocognitive decline … there is literature showing concern for hydrophilic with increased disease progression in PD.
I’m not sure what to choose for that as it’s a decision under uncertainty. Initially Attia and Dayspring had a preference of hydrophilic statins as they believed it had a lower probability of passing the BBB and reducing desmosterol of which reduced levels are at least associated with MCI. Later on at least Dayspring have said all statins cross the BBB, so it is a bit moot for AD.
Attia looked at many statin trials and they all had a neutral or positive effect on secondary outcomes for dementia IIRC. APOB seems causally linked with AD based on MR studies. So they seem positive in general (except possibly in the scenario where serum desmosterol lowers too much, especially in apoE4 carriers).
adssx maybe knows better about PD, but it seems lipophilic statins are better for this (?).