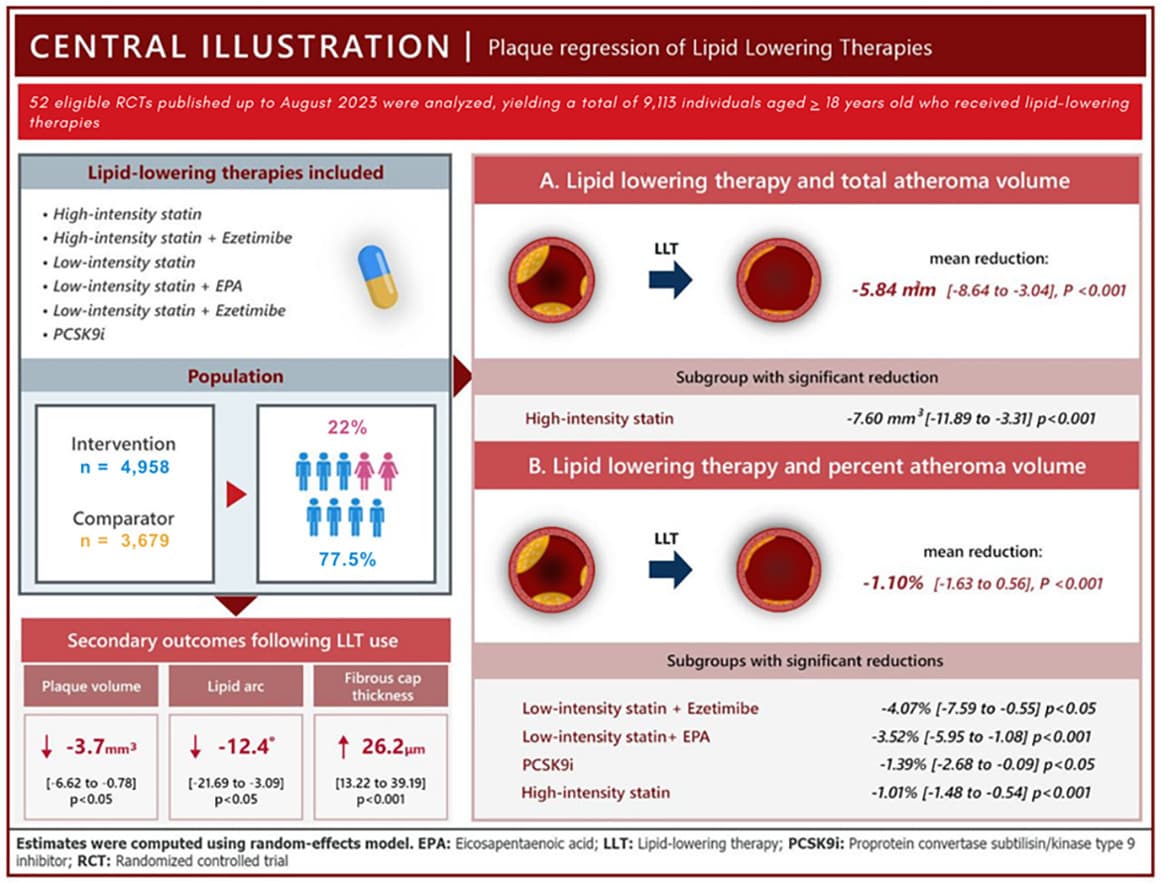
while the addition of ezetimibe seemed to significantly increase the PAV reducing effect of LIS while decreasing the PAV reducing effect of HIS, these inconsistent results were driven by the significant heterogeneity in the LIS plus ezetimibe subgroup (τ2 = 0.88, I2 = 61.8%), and possibly the limited number of included studies in the HIS plus ezetimibe subgroup. In fact, previous studies demonstrated that the addition of ezetimibe do not contribute to a significant increase in PAV reduction. While the role of statins on plaque regression have been discussed above, we emphasize that HIS was the only LLT subgroup which provided significant reductions in both TAV and PAV.
Perhaps, the more significant finding of our study in PAV reduction is the role of EPA. […] While many previous studies have demonstrated that the addition of EPA to statin contributes to increased plaque regression, our pooled analysis showed that the addition of EPA to LIS is superior even when compared to other multiple classes of LLTs, supporting the hypothesis that EPA contributes to plaque regression in mechanisms beyond lipid-lowering, giving emphasis to the role of its anti-inflammatory effects in plaque regression. However, the question on whether the overall results translate to a clinically meaningful reduction still remains.
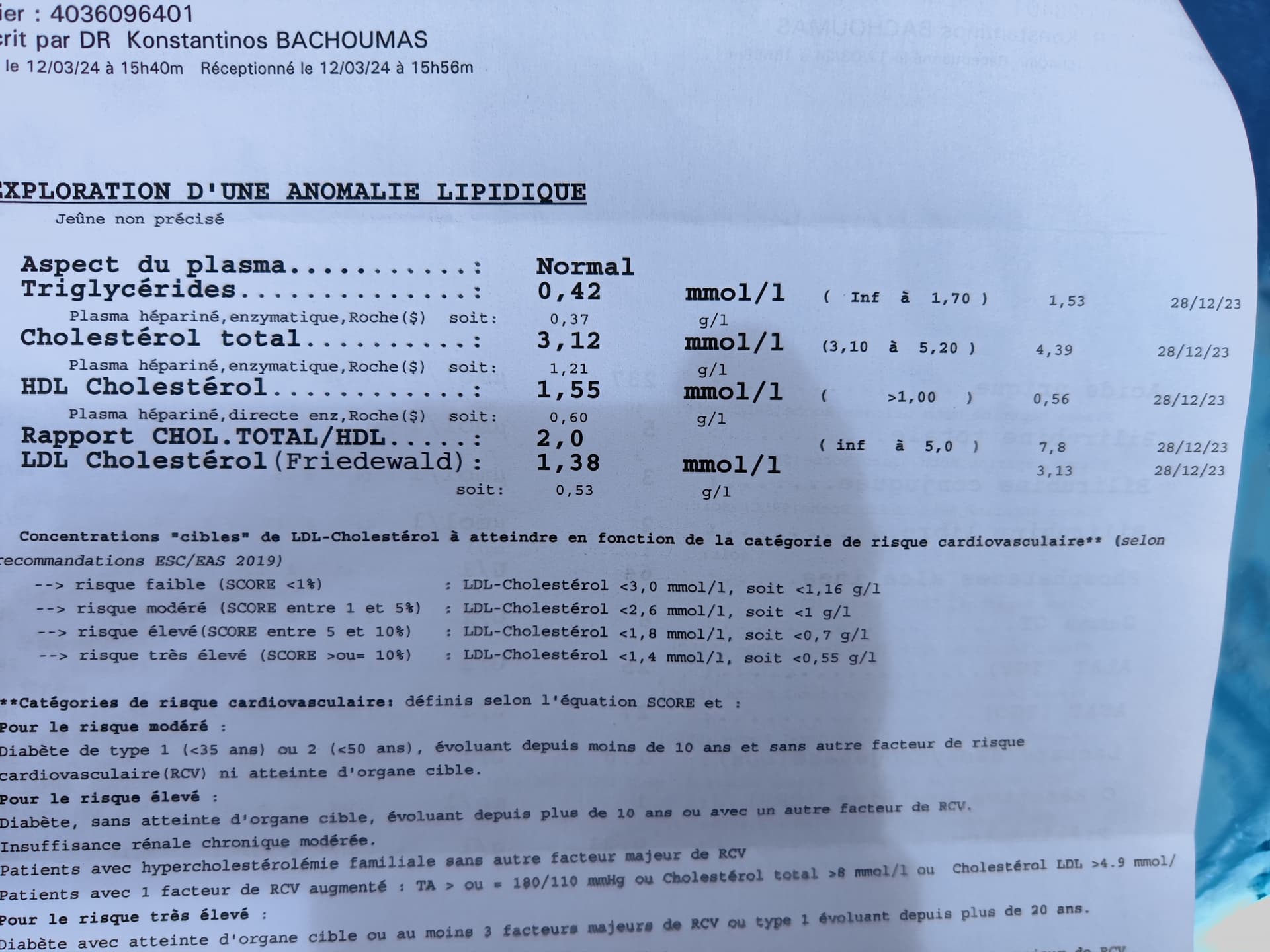
They didn’t define LIS and HIS though
Bempedoic acid not included in the review. Would be interesting to test low-intensity statin + ezetimibe + EPA (+ bempedoic acid?). Or just wait for obicetrapib…
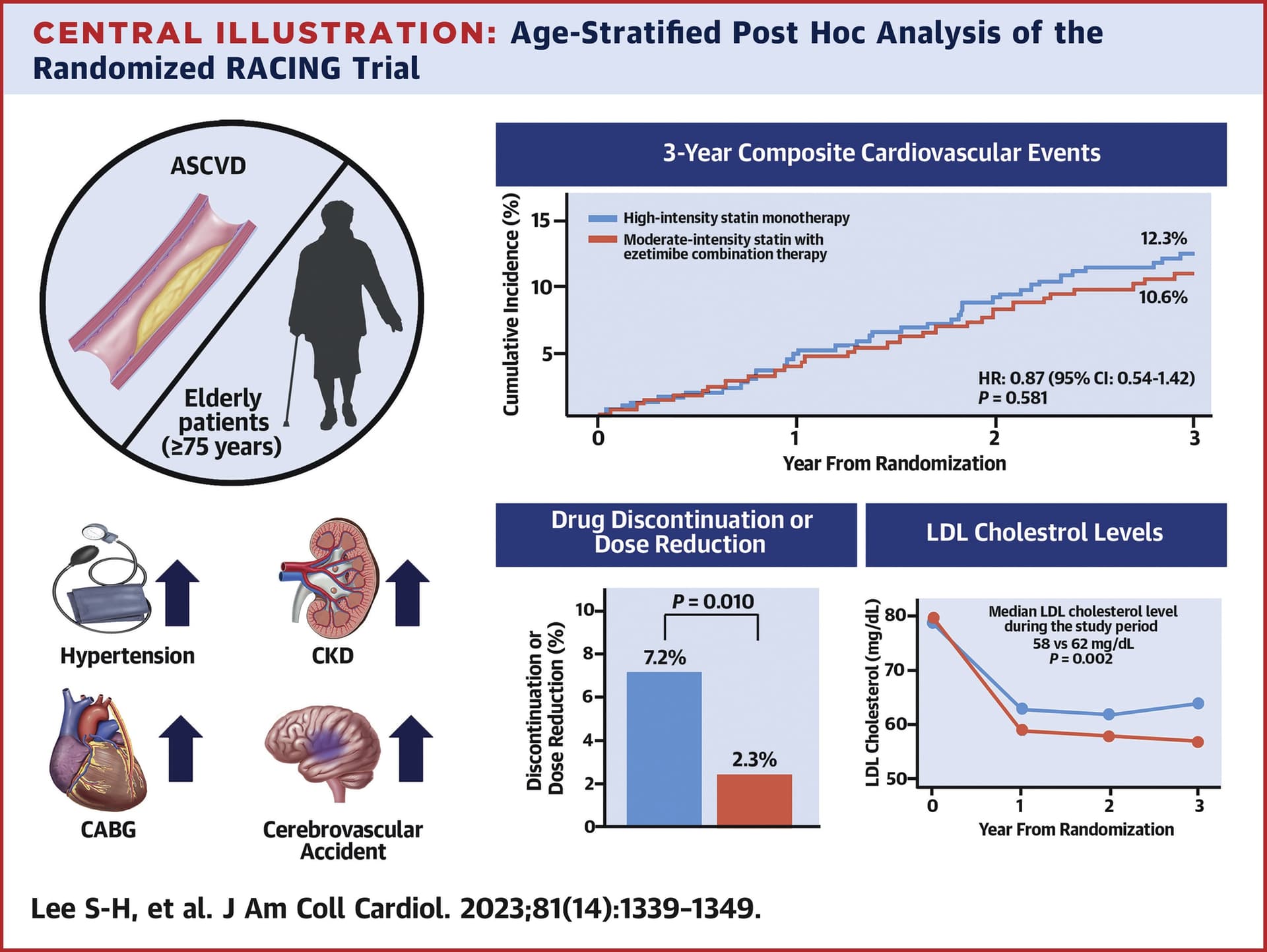
I think this is particularly notable: " Compared to high-intensity statin monotherapy, moderate-intensity statin with ezetimibe combination significantly reduced the risk of composite outcome [hazard ratio (HR) 0.84, 95% confidence interval (CI) 0.77–0.92, P < 0.001]"
I was on Lipitor, but stopped because of muscles pain. Now I’m on 5mg Rosuvastatin every other day, alternating it with 10 mg ezetimibe. Works great for me with no muscle pain, and it does lower lipids gradually. Doesn’t affect my glucose level as well.
Yes but I would have to look at the largest clinical trials, I have heard they have detected an improvement in cardiovascular mortality (but not all-cause) and the MR studies you posted before will help. I don’t know what to think of higher doses of atorvastatin either.
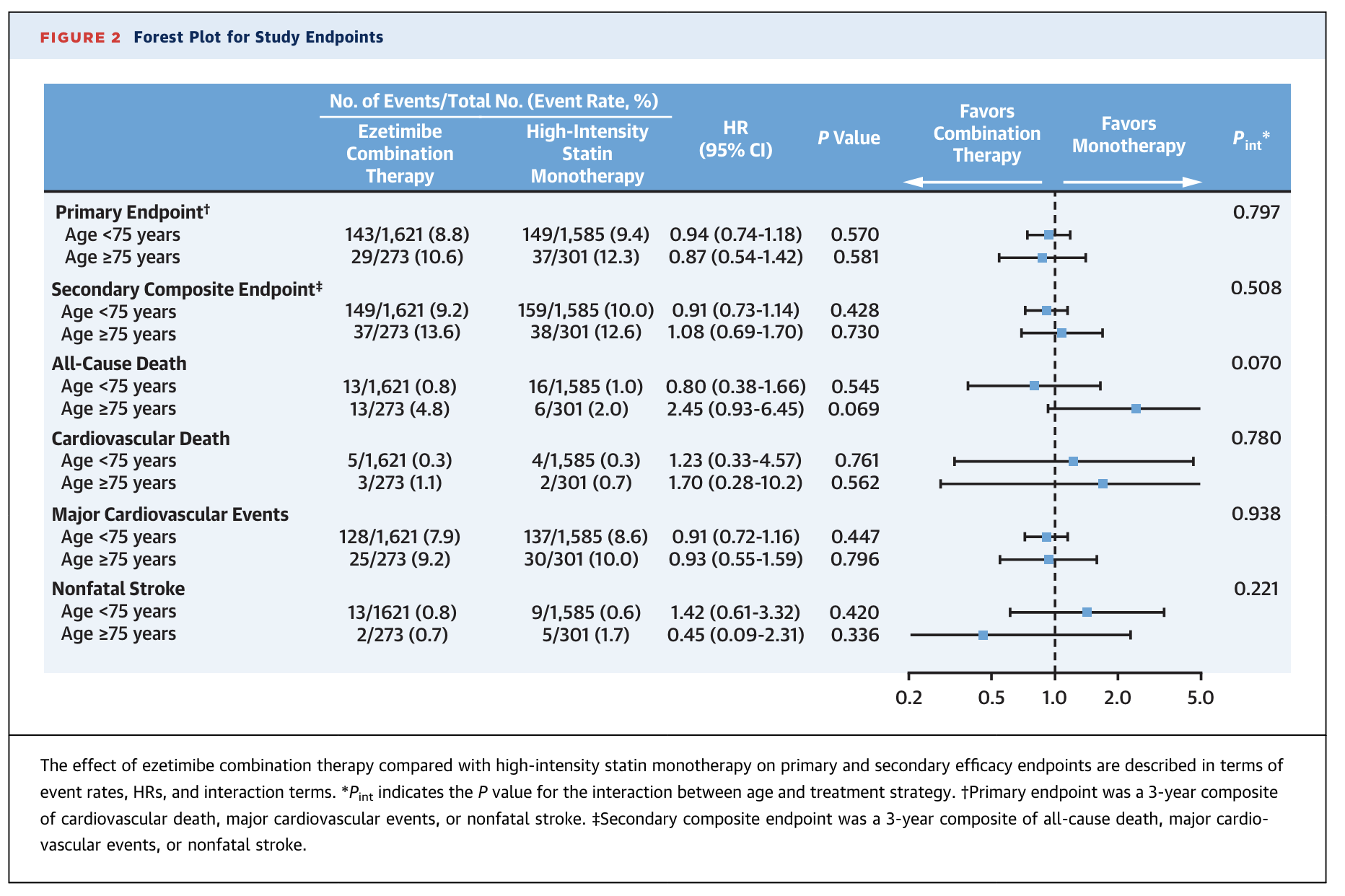
Third, the rate of the all-cause death was numerically higher in the ezetimibe combination therapy group than in the high-intensity monotherapy group among patients aged >=75 years. However, the difference was not significant, and the comparison of individual component of the primary or secondary composite endpoint was difficult because of the small number of events; therefore, the results should be interpreted with caution.
We don’t know whether ezetimibe caused the trend towards slightly higher acm or whether high intensity statin usage caused a lower acm compared to combination therapy. If it’s the latter, combined high intensity statin therapy and ezetimibe would yield even better results.
Simvastatin may be best if you are worried about MS.
Simvastatin (Flolipid, Zocor) is a statin doctors prescribe to treat high cholesterol. It may also help slow down secondary progressive MS. Some studies show that higher cholesterol levels are linked to worsened MS. Because of this, experts thought simvastatin might slow down MS progression if it lowers your cholesterol. But a more recent study found that the drug directly slows down the progression of MS, even if it doesn’t help your cholesterol levels.
Our results suggest that beneficial effects of simvastatin on reducing the rate of brain atrophy and slowing the deterioration of disability are independent of serum cholesterol reduction.
That might be helpful for aging brains more generally.
Only one specific type of MS, but as of Sep 20, this year:
A phase 3 trial revealed that simvastatin, while safe, did not significantly slow disability progression in patients with non-active secondary progressive MS.
However,
However, … , an Italian research team went back to reassess disability levels in 69 participants 8 years later. They found that taking atorvastatin (20 or 40 mg/day) in combination with beta interferon for 2 years in the original study was linked to milder disease progression 8 years later. The researchers suggest that statins may slow down progression in MS, but there may be a lag in the effect. However, this was just a small group from the original study; of the 69 reassessed, 42 had taken beta interferon plus placebo and just 27 had taken beta interferon plus atorvastatin.
Wrt. the title of this thread, I’m embarking on an experiment. I’m switching from 10mg/day atorvastatin to 4mg/day pitavastatin. I tolerated the atorvastatin very well for the roughly 5 years I’ve been taking it, but with every passing year, it has been less and less effective at lowering my LDL, best was first year, LDL 70, and worst this year, just got my results, LDL 146. Clearly, I had to do something. My PCP suggested upping the atorvastatin to 20mg/day, but as most of the lipid lowering effect is at the lowest dose, I wasn’t enthusiastic about pushing on the same string. So, I’m going to try a different statin. Monday 10/29 was the last day of my atorvastatin, and I’m taking three days off to allow any trace of atorvastatin to be eliminated, and I’m starting on pitavastatin 4mg/day Friday night. How I will tolerate it, and the impact on my lipid profile ApoB etc., I’ll have to see. There are many comparison studies showing PIT as superior to ATO and other statins wrt. primary MACE endpoints, but found lipoprotein lipase interesting: