In the phase 2 trial, after 8 weeks, obicetrapib 10 mg reduced ApoB by 29.8%, non-HDL by 44.4% and Lp(a) by 56.5% and increased HDL by 165% and apolipoprotein A-I by 47.8% (P for all < .0001). (source)
We identified six lipid-lowering variants that were associated with increased lifespan, including PCKS9 (Beta 0.11; 95% CI: 0.06 to 0.15; p-IVW=4.55×10-6, FDR=5.95×10-5), CETP (Beta 0.24; 95% CI: 0.14 to 0.34; p-IVW=3.72×10-06, FDR=5.31×10-5), APOC3 (Beta 0.08; 95% CI: 0.04 to 0.12; p-IVW=4.67×10-5, FDR=4.58×10-4), LDLR (Beta 0.15; 95% CI: 0.11 to 0.19; p-IVW=1.08×10−11, FDR=2.83×10-10), and LPL (Beta 0.12; 95% CI: 0.09 to 0.195; p-IVW=1.62×10-15, FDR=8.48×10-14). There was little statistical evidence of longevity-associated effects among NPC1L1 (Beta 0.06; 95% CI: -0.16 to 0.28; p-IVW=0.58, FDR=0.76) and HMGCR (Beta 0.08; 95% CI: 0.01 to 0.15; p-IVW=0.03, FDR=0.11).
The genetically proxied CETP and APOC3 inhibitions also showed causal effects on increased life expectancy in both outcome datasets. The lipid-lowering variants of HMGCR, PCKS9, LPL, and APOB were associated with longer lifespans but did not causally increase extreme longevity. No statistical evidence was detected to support an association between NPC1L1 and lifespan.
(same authors, too bad they didn’t look at gender differences though)
We actually discussed it a few times in 2023 so might want to see if anything valuable from those past discussion for you
Also Peter Attia had a Drive episode with one of the top guys involved with the trials (the fall or so of 2023 so relatively fresh), so might want to check that out.
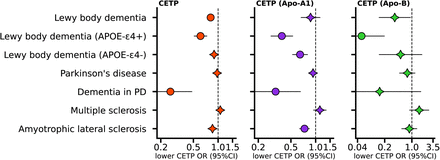
Consideration of dementia related traits indicated that lower CETP concentrations were associated higher total brain volume (0.04 per standard deviation, 95%CI 0.02; 0.06), lower risk of LBD (OR 0.81, 95%CI 0.74; 0.89) and Parkinson’s dementia risk (OR 0.26, 95%CI 0.14; 0.48).
For now the trials are only on top of high statin dose for uncontrolled hyperlipidemia. So unless they do new trials to show that they can replace statins as first line treatment I would assume the price to be similar (per year). Maybe a bit lower as it’s a pill so they can expect more sales (I assume that they want to reach the same revenue and are okay to lower the price if that means more sales). So about €/$/£10k/y?
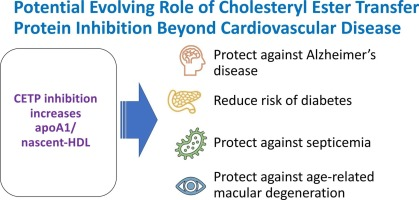
Although RCTs have shown mixed results regarding the impact of CETPi on cardiovascular disease, they have shown a consistent reduction in the risk of new-onset diabetes with CETPi therapy. Future trials of CETPis and potentially other HDL-raising agents should therefore specify new-onset diabetes and reversal of existing T2DM as secondary endpoints.
Our findings suggest that CETP inhibitors, which are currently in clinical trials to treat cardiovascular disease, can be repurposed to treat metabolic disease in a combination therapy approach with SGLT2 inhibitors.
(synergistic effects with SGLT2i )
If confirmed, I understand that obicetrapib would be the only lipid-lowering drug that also increases insulin sensitivity (others are either detrimental or neutral) and prevent dementia (others either have detrimental effects on cognition or are neutral). Huge if true… (and I would be the first customer to buy it…)
In PD, statins cause faster neurological decline (per RCT + MR + longitudinal studies). In healthy people, the picture is less clear, and there’s conflicting data, but at least I think we can agree that by raising blood glucose they might have a negative effect on cognition. Whether this is a net positive or net negative probably depends on your pre-treatment LDL & ApoB levels. So on that point for sure, a lipid-lowering drug that increases insulin sensitivity would be amazing.
“Our results of higher HDL-C and mainly its small HDL-C subfraction suggest that male MS patients are at higher risk of atherosclerosis and the subtle dyslipidemia is present in early stages of the disease. The correlations between specific HDL-C subfractions and the inflammatory cytokines demonstrate mutual links between systemic inflammation and lipid metabolism in MS.”
“Fingolimod and DMF therapies are associated with a specific increase in HDL in PwMS. Further studies are required to validate these findings and their potential implication as biomarker of reduced inflammatory state and/or reduced risk of neurodegeneration or cardiovascular comorbidity.”
“TC to HDL-C ratio is associated with MS fatigue. Our results implicate a potential role for the HDL-C pathway in MS fatigue and could provide possible targets for the treatment of MS fatigue.”
“The relative proportions of low density cholesterol to high density cholesterol were associated with cognitive performance speed as measured on the symbol digit modalities test (SDMT).”
Based on solid evidence from studies with isolated macrophages, rodents, and humans, we propose that a major function of CETP may be to modulate HDL in order to help resolve bacterial infections. When gram-negative bacteria invade the blood, as occurs in sepsis, Kupffer cells lose their expression of CETP to increase HDL levels. This rise in HDL prevents systemic endotoxemia by binding lipopolysaccharide and induces a systemic proinflammatory response in macrophages to mediate bacterial clearance. This raises the interesting possibility to repurpose CETP inhibitors for the treatment of sepsis.
This is unfortunately nonsensical wishful thinking. The price of a drug is unrelated to its production cost. Ravicti costs nothing and is sold $600k/y. Relyvrio for ALS costs $158k/y even though it’s just the combination of one generic and one cheap Chinese medicine supplement that you can buy on Amazon.
If it costs a lot to produce it will be priced higher to the customer to have the same profit.
There exists a significant unmet need for a potent, cost-effective and convenient LDL-
lowering therapy as an adjunct to statins, a class of lipid-lowering medications that are the current
standard of care for high-risk CVD patients with high cholesterol.
Cost-effective for payers. PCSK9 are expensive but cost effective VS apheresis for those who have it. So here it’s probably indeed cost effective VS PCSK9i. So less than $5k/y? Bempedoic acid/ezetimibe costs about $2k/y, I would assume obicetrapib will cost more.
So either they want to sell at a price just below PCSK9i but sell 10x more. Of they want to sell it at a higher price.
But for now they haven’t started trials on obicetrapib VS statins as first line treatment. They only looked at uncontrolled dyslipidemia despite max statin dose. That’s a smaller market so they need a higher price point to reach their 4bn revenue goal.
I have a ridiculous argument, but technically if it only costs $35 a year to produce they could sell it at 3 billion divided by 35 M patients, from same source I linked above:
We estimate that there are approximately 35 million patients in the United States and EU5 who
are not achieving LDL-lowering goals on current standard of care.
Which is 85 + 35 = $120 / year to the patient. That would be the best option as they make their money and allow as many people as possible reach their target. If I remember correctly anyone could manufacture this. I don’t know what pharma companies typically choose to do.
Interesting that the papers above generally paint the picture that
“Higher HDL-C levels are associated with decreased disease activity.”
“Higher LDL-C levels are associated with increase disease activity.”
“Immunomodulatory treatment has positive effect on lipid profile in multiple sclerosis.”
Below is an MR on LDL and HLD potential effect on MS that in someways is more similar to the CETP MR analysis
(Btw it also suggests that statin’s non lipid lowering effects might be positive for MS).
Exploring the Role of Plasma Lipids and Statin Interventions on Multiple Sclerosis Risk and Severity: A Mendelian Randomization Study
Results: The results of MR using the inverse-variance weighted method show that genetically predicted RAC2, a member of cholesterol-independent pathway (OR 0.86 [95% CI 0.78-0.95], p-value 3.80E-03), is implicated causally in reducing MS risk. We found no evidence for the causal role of LDL-C and the member of cholesterol biosynthesis pathway on MS risk. The MR results also show that lifelong higher HDL-C (OR 1.14 [95% CI 1.04-1.26], p-value 7.94E-03) increases MS risk but TG was not. Furthermore, we found no evidence for the causal role of lipids and genetically mimicked statins on MS severity. There is no evidence of reverse causation between MS risk and lipids.
Discussion: Evidence from this study suggests that RAC2 is a genetic modifier of MS risk. Because RAC2 has been reported to mediate some of the pleiotropic effects of statins, we suggest that statins may reduce MS risk through a cholesterol-independent pathway (that is, RAC2-related mechanism(s)). MR analyses also support a causal effect of HDL-C on MS risk.
It should be legal to make your own obicetrapib at home, unless the precursors, etc aren’t, so that could be an option. I hadn’t thought about that. Wouldn’t the equipment be expensive though?