Grey peptides are amazing when you know where to order. Cheaper than pharma and effective.
(WWB)China Price list 12-23.pdf (200.2 KB)
4 Likes
When it says “WWB”, is that World Well-Being ?
1 Like
No, that is something else.
1 Like
Wuhan something I believe
Yes like COVID lol
1 Like
8 Likes
Yes, but you have no idea on the contaminants levels, and other issues. See this thread: ‘I wouldn’t dare take these drugs’: how China supplies untested peptides to the west (Financial Times)
2 Likes
Phenomenal analysis and discussion of this Lilly result from The Incretin Space:
7 Likes
Yes, contaminants could be a real problem but it seems to me that everybody must synthesize peptides in a similar if not identical way. And, peptides are macro-molecules so purifying them by dialysis or by exclusion columns would seem to be cheap, easy, and routine. All this to say that I wonder if contaminants are as big of a problem as people think?
It would be nice to see a study of random grey market peptides from various sources to determine what the contaminants are and how prevalent the problem. Peptide identity and degradation or partial synthesis products would seem to be a more likely variable.
4 Likes
I’m imagine someone here knows this….
Has there ever been a case of someone getting sick from a grey market peptide when it came from a batch tested by Janoshik (or similar)
Vs someone buying from an unknown source on TikTok, forum, or going to a random spa etc?
Multi-omic profiling reveals Retatrutide alleviates adipose tissue fibrosis via metabolic reprogramming and tissue repair
Summary:
- Weight and Fat Reduction : retatrutide specifically reduced the mass of epididymal, inguinal, and interscapular brown adipose depots.
- weight loss was driven by enhanced energy expenditure rather than chronic appetite suppression, as food intake did not significantly differ between the HFD and Retatrutide-treated groups during the intervention.
- Multi-omic analysis of epididymal WAT (eWAT) revealed that Retatrutide transforms “sick” fat into a metabolically active organ through several coordinated processes:
– shifted the transcriptional landscape from lipid storage to lipid oxidation
– suppressed pro-fibrotic signaling pathways (TGF-β, focal adhesion) and reduced collagen-derived metabolites. It also attenuated broad-spectrum pro-inflammatory genes and pathways (NF-κB, Toll-like receptor signaling) while restoring anti-inflammatory immunoregulatory genes.
– promoted tissue repair by upregulating pro-homeostatic and angiogenic markers
– restored mitochondrial membrane integrity and peroxisomal activity, both of which are typically compromised in obesity.
3 Likes
I have NEVER heard someone getting sick from buying/using grey market peptide, NEVER. I have bought and used about 30 peptides (all useless btw) from probably 10 different gray/black market suppliers, and I have never gotten sick from using these peps. Having said that there was a case in LV where couple people were injected with supposedly some kind of peptide and ended up in the hospital, but who knows what they were injected with, plus that doesn’t count as gray since they were literally administered the injection while taking part in some sort of peptide convention or something similar. To each their own but I have little sympathy for those that show up at a hotel somewhere and let a stranger inject stuff into their bodies. So, I don’t think this counts as gray market stuff.
4 Likes
That’s interesting, as I’ve heard Reta doesn’t have to suppress appetitie, while it’s annihilating mine currently. Maybe that’s the signal that it’s too high a dose
The dosages for non diabetic/non obese longevity users might be different than the doses used for those who are sick - I’m learning
I pushed it to 6mg, probably stupidly, and after a month still can’t look at food when I was already losing strongly at 4mg and my blood pressure and glucose were already down
I had that 8mg in my mind as what some consider “therapeutic dose”
1 Like
Therapeutic dose starts at 4mg. 8mg is one of the doses that had major weight loss. 12mg was better, but not by much. Some people think glucagon only kicks in at higher doses, but pre clinical data shows that you get glucagon activation at low doses.
Over time, you’ll find that your appetite returns, but that you keep losing weight.
3 Likes
Does the appetite always return under all doses?
Does the body get used to all doses?
One of the reasons I titrated up to 6, in addition to wanting to get to the 8-12 range that saw the most dramatic results in weight change and I’m guessing metabolic/anti inflmmatory change (aren’t a lot of the changes dose dependent?), is that I felt my appetite was back after a month of 4mg… Now after a month of 6mg still waiting for some equilibrium in terms of side effects…
If it continues I will just retreat to 4mg
1 Like
Appetite returns, yes. If you browse GLP1 related forums, you’ll see posts about people panicking/complaining about lack of appetite surpression after being on a dose for awhile (mostly tirzepatide, semaglutide but this applies to all GLP1a) . They’re often worried about gaining the weight back since they’re eating more, but what ends up happening is that although they may not be losing more weight, they’re maintaining their weight loss.
I would increase the dose only on a weight loss plateau (4 weeks of no weight loss), not on loss of appetite suppression.
Your body gets used to a dose over time, if you’re talking about side effects . I’ve been on the same high dose for 4 months, and I’ve had 0 side effects on that dose, while slowly losing more weight. My appetite has been pretty normal during that period.
You can always monitor some changes via a metabolic panel. I saw my markers improve early when I was on only 4mg: decrease on A1c, Triglycerides, and better egfr.
1 Like
I haven’t been losing weight slowly… I’ve been on the med for a little over 3 months and went from ~198 to ~162…
This might be part of the issue…
I increased the dose even while running through the weight, having dizziness etc
I may need to take a step back and think its working too well for me… and need to be more selective with titrating up…
I’m seeing the trials and they are talking about 12mg for mass weight loss when it was heading that way for me on low dosage…
I suspect that I take a lot of glycine is at issue… it has glp affects which can be additive I’m thinking and folks often take glycine with these meds
Thats good, having this conversation made it obvious to me what my next move should be, lol.
I just though I saw some dose dependent reports that made me want to shoot for the stars.
3 years ago, the obesity drug market was basically Ozempic. Today, it’s 9 drugs deep in late-stage. Here’s what each one actually adds:
Foundayo: latest oral GLP-1. approved April 1, 2026. Injections become optional.
Retatrutide: 24% weight loss at 48 weeks (Phase 2). Triple agonist.
CagriSema: less nausea than semaglutide. NDA filed December 2025.
Survodutide: GLP-1 + glucagon. Cuts liver fat alongside weight.
Amycretin: oral weekly. GLP-1 + amylin. Phase 2.
Petrelintide: amylin only. Phase 2 posted March 2026.
Mazdutide: China approved 2026. US Phase 3 ongoing.
Pemvidutide: obesity + MASH dual indication.
Monlunabant: CB1 inverse agonist. Phase 2.
The next pharma cycle may not be Novo vs Lilly. It’s shaping up as mechanism vs mechanism.
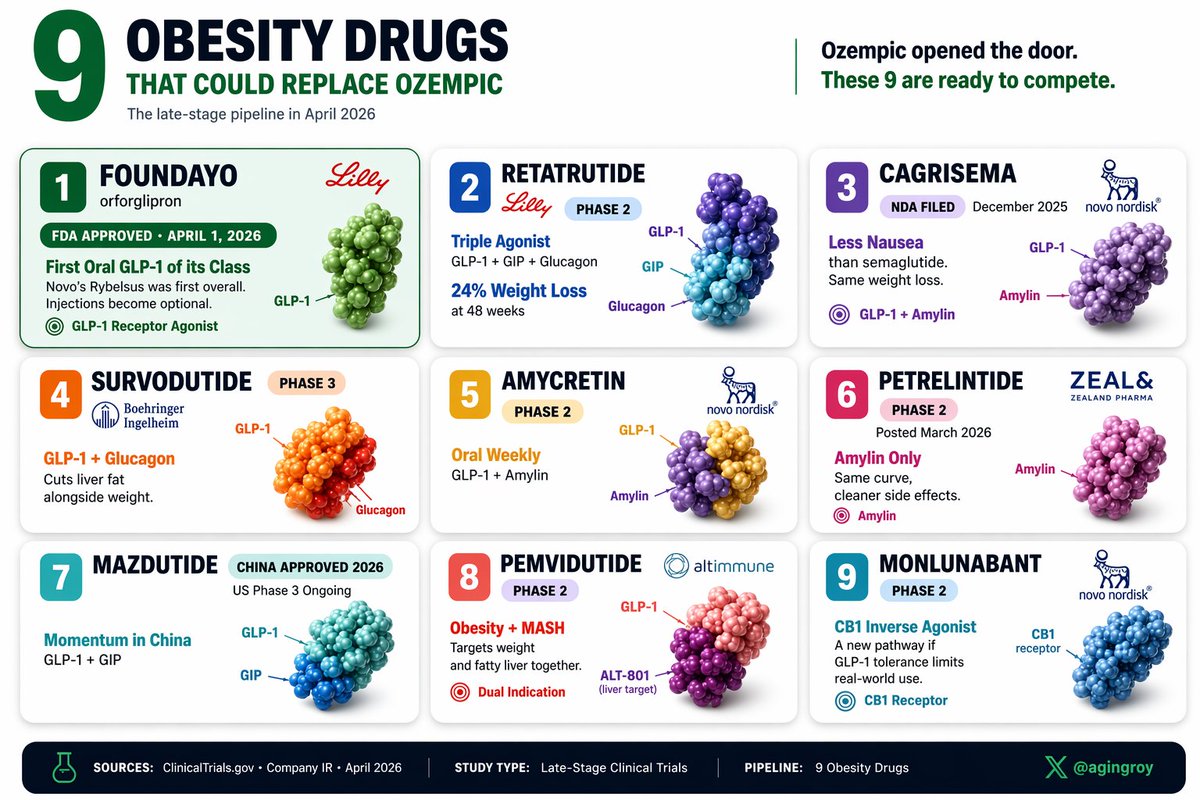
Source: https://x.com/agingroy/status/2045551011612500182?s=20
6 Likes
Hi
For the people on retatrutide here, do you have the skin burning sensation/itching? It’s so annoying when you try to sleep. It’s really a weird sensation. I’m week 1 on 8mg a week.
It’s not a histamine problem I’m already take 5mg of desloratadine daily.
Thanks
1 Like
Reta ‘can cause skin-related discomfort known as allodynia or dysesthesia, which is described as heightened sensitivity, burning, tingling, or pain from light touch. Roughly 7–21% of users in high-dose studies reported this, often described as a sunburn-like sensation, which is typically temporary and dose-dependent.’
I’ve never had it but some suggest a zinc supplement helps. I suspect the zinc doesn’t do much and it’s just people having the effect diminish because some time has gone by as it’s often temporary.
6 Likes