Researchers gave aging mice five months of low-dose dietary rapamycin — the same “gold-standard” longevity drug and dosing protocol used in the landmark NIH Interventions Testing Program studies — and then took a careful census of the aging immune system. The headline surprise is what didn’t happen: rapamycin left the broad architecture of the immune system essentially untouched (no myeloid skewing correction, minimal B- and T-cell changes, no change to resting brain microglia). What it did do was surgically suppress one specific troublemaker — the age-associated expansion of IL-17-producing gamma delta (γδ) T cells, especially in the abdominal cavity — and blunt the inflammatory storm (including brain microglial activation) when the mice were later hit with a bacterial toxin challenge. The paper reframes rapamycin less as a blunt immunomodulator and more as a targeted dampener of a specific inflammaging circuit linking the periphery to the brain.
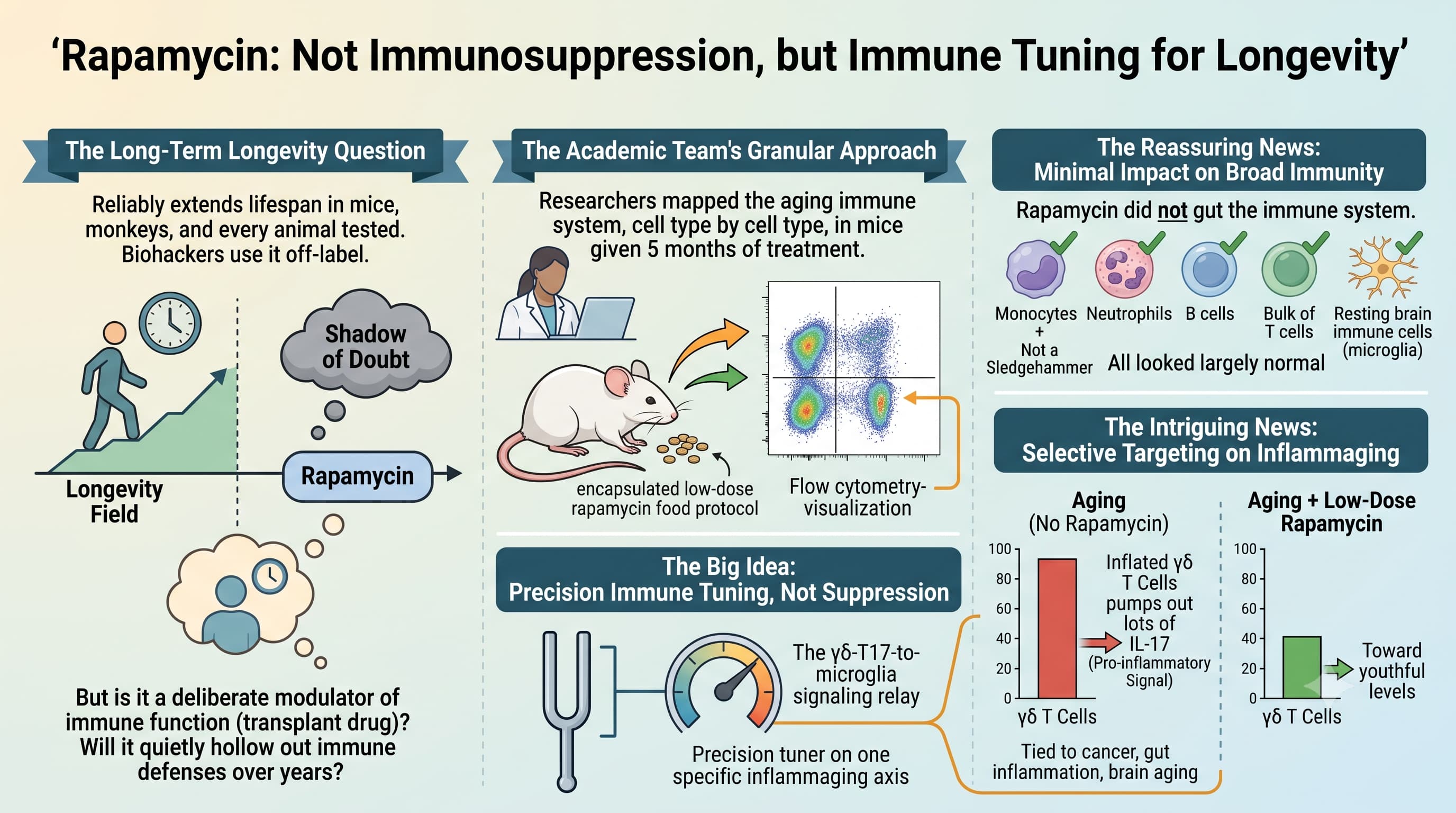
Rapamycin has spent two decades as the poster child of the longevity field. It reliably extends lifespan in mice, monkeys, and every other animal its been tested on, and tens of thousands of committed biohackers already take it off-label. Yet a small worry has shadowed the drug: rapamycin is, first and foremost, a transplant drug — a deliberate modulator of immune function. If you take it for years, even at low, periodic dosing to slow aging, some people have wondered if you quietly lowering the very immune defenses that keep an older body alive?
A team spanning the German Center for Neurodegenerative Diseases (DZNE) in Bonn, Barts Cancer Institute in London, and University College Cork set out to answer this directly. Rather than measure survival, they did something more granular: they mapped the aging immune system, cell type by cell type, in mice given five months of the exact low-dose, food-encapsulated rapamycin protocol pioneered in the famous lifespan-extension trials.
The reassuring news is how little broke. Rapamycin did not gut the immune system. Monocytes, neutrophils, B cells, and the bulk of T cells looked largely normal. Resting brain immune cells (microglia) were unchanged. This is not the profile of a drug carpet-bombing immunity.
The intriguing news is what it selectively hit. Aging normally inflates a population of γδ T cells that pump out interleukin-17 (IL-17), a pro-inflammatory signal increasingly tied to cancer, gut inflammation, and brain aging. Rapamycin pushed those cells back down toward youthful levels — most clearly in the peritoneal (abdominal) cavity. Then, when the researchers challenged the animals with LPS (a bacterial toxin that triggers a body-wide inflammatory response), the rapamycin-fed mice mounted a measurably cooler response: lower circulating IL-17, IL-12p40, and IL-27, and a calmer inflammatory gene signature in brain microglia.
The Big Idea is a shift in how we think about rapamycin’s benefit. Instead of a sledgehammer that suppresses everything, this work strongly suggests rapamycin acts as a precision tuner on one specific inflammaging axis — the γδ-T17-to-microglia signaling relay that may connect a low-grade inflamed body to a low-grade inflamed brain. If that relay is causal in age-related neuroinflammation, then rapamycin’s much-discussed brain benefits might run partly through the immune system, not only through neurons directly.
The caveats are substantial: this is a small mouse study, it measured immune phenotypes rather than disease outcomes or lifespan, the LPS experiments used females only, and the peripheral-to-brain link remains correlational. But as a mechanistic clue, it is a genuinely useful one.
Actionable Insights
The take-home signals:
1. Rapamycin at a longevity dose looks immunologically “quiet,” not immunosuppressive. The most decision-relevant finding for people already weighing rapamycin is a reassurance signal: at the Harrison/ITP low dose (~14 ppm active, ~2.24 mg/kg in mice), broad immune cell populations — including neutrophils and B cells that guard against infection — were essentially unchanged over five months. Effect size: qualitatively null across most measured populations (differences did not reach significance; the authors report only p < 0.1).
2. The benefit is targeted, not global. The one robust hit was suppression of age-expanded IL-17-producing CD27– γδ T cells, “rescued” toward young levels in the peritoneal cavity. Because the paper publishes only figures (mean ± s.e.m.) and p-values below 0.1 — not source numbers — a precise Cohen’s d cannot be honestly calculated from the text. The described effect is a partial-to-full normalization of an age-driven increase (directionally large, but the real-world magnitude is not quantifiable from the reported data).
3. Context matters more than baseline. Rapamycin’s anti-inflammatory effect only became visible under an inflammatory challenge (LPS), not at rest. Translation for humans: any such benefit would likely matter most during infection/immune stress — precisely the setting where immunosuppression is also the biggest theoretical risk. That tension is unresolved at some level, but from a practical standpoint this is rarely an issue. Unlike in most of these mouse studies where the rapamycin is dosed continuously with food, people using rapamycin for longevity typically take rapamycin on a pulsatile dosing schedule (only one dose per week or once every two weeks, etc.), so any immune system impact is likely to be short.
Context / Source
- Open Access Paper: Long-term rapamycin treatment suppresses IL-17-producing gamma delta T cells and blunts neuroinflammation in aging.
- Authors: Torrent C, Gagliardi C, Fülle N, Antignano I, Bernis ME, Stork M, Bano D, Capasso M, Keane L.
- Lead institutions: German Center for Neurodegenerative Diseases (DZNE), Bonn, Germany; Barts Cancer Institute, Queen Mary University of London, UK; University College Cork, Ireland.
- Journal: PLOS ONE, 2026; 21(5): e0343183. Published May 28, 2026.
- Impact evaluation: The impact score of this journal is 2.8 (2025 Journal Impact Factor; CiteScore ≈ 3.4), evaluated against a typical high-end range of 0–60+ for top general-science journals, therefore this is a Low-to-Medium impact journal.