I’m a 70 yr old male living with HIV for the past 12 years. I’ve been reading about Rapamycin and have ordered some. Excited about the benefits.
Here is a confusing concept for me: autophagy.
I understand (correctly?) that Rapamycin increases autophagy. Nigella Sativa, on the other hand, is reported to inhibit it. But Nigella Sativa has so many benefits, according to all of the studies I’m reading.
Will these two substances counteract each others’ benefits? Do I have to choose between anti cancer and longevity>
Thank you, Sir. I look forward to a better understanding. Nigella Sativa sounds like a miracle substance, like Rapamycin. I hope I’ll get some responses from others who share my curiosity, and even some who are living with HIV. John
Nutritional Value and Preventive Role of Nigella sativa L. and Its Main Component Thymoquinone in Cancer: An Evidenced-Based Review of Preclinical and Clinical Studies
Review on Clinical Trials of Black Seed (Nigella sativa ) and Its Active Constituent, Thymoquinone
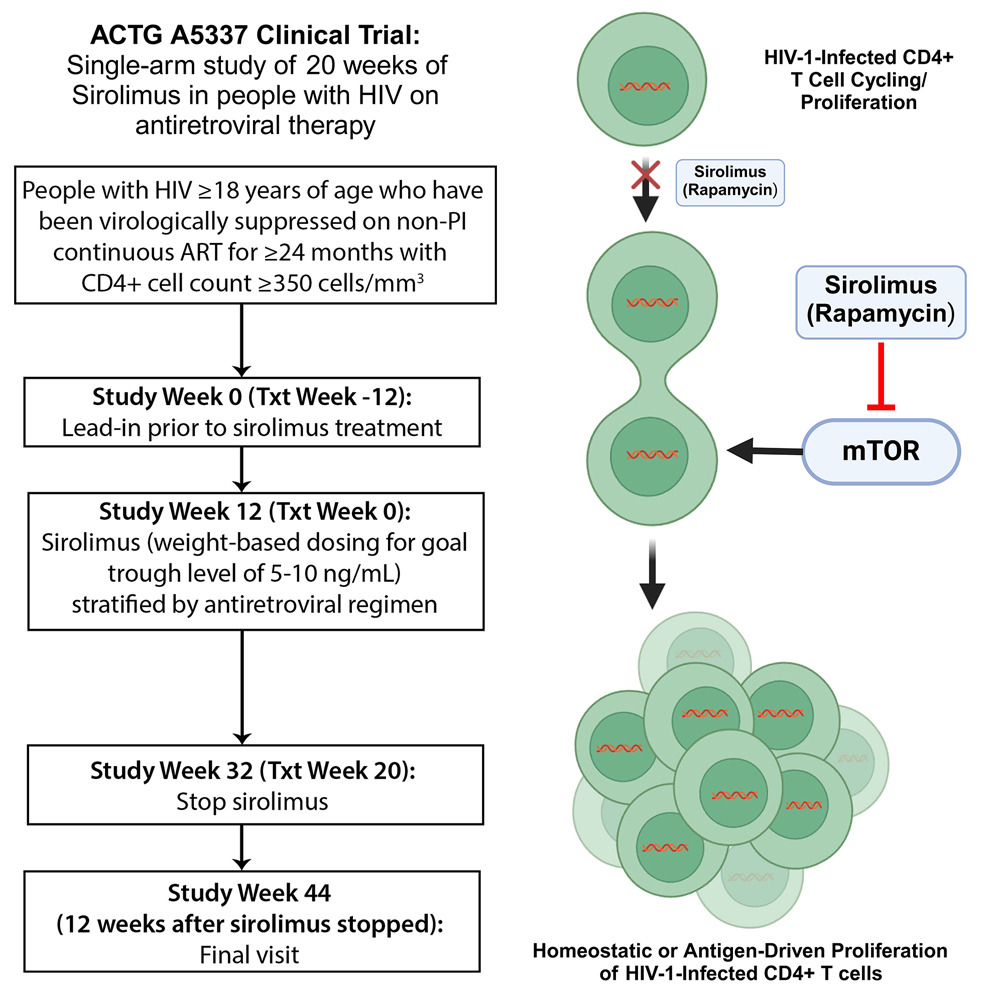
Sirolimus (rapamycin) reduces HIV-1 proviral DNA by reducing homeostatic cell cycling of infected CD4+ T cells
Highlights
• Sirolimus treatment decreases cell-associated HIV-1 levels in people with HIV on ART
• The reduction in HIV DNA persists for at least 12 weeks following sirolimus treatment
• Sirolimus reduces CD4+ T cell cycling and CD8+ T cell PD-1 expression
• Sirolimus does not impact HIV-1-specific CD8 T cell responses or HIV-1 RNA levels
Summary
Key HIV cure strategies involve reversing immune dysfunction and limiting the proliferation of infected T cells. We evaluate the safety of sirolimus, a mammalian target of rapamycin (mTOR) inhibitor, in people with HIV (PWH) and study the impact of sirolimus on HIV-1 reservoir size and HIV-1-specific immunity in a single-arm study of 20 weeks of treatment in PWH on antiretroviral therapy (ART). Sirolimus treatment does not impact HIV-1-specific CD8 T cell responses but leads to a significant decrease in CD4+ T cell-associated HIV-1 DNA levels at 20 weeks of therapy in the primary efficacy population (n = 16; 31% decline, p = 0.008). This decline persists for at least 12 weeks following cessation of the study drug. Sirolimus treatment also leads to a significant reduction in CD4+ T cell cycling and PD-1 expression on CD8+ lymphocytes. These data suggest that homeostatic proliferation of infected cells, an important mechanism for HIV persistence, is an intriguing therapeutic target.