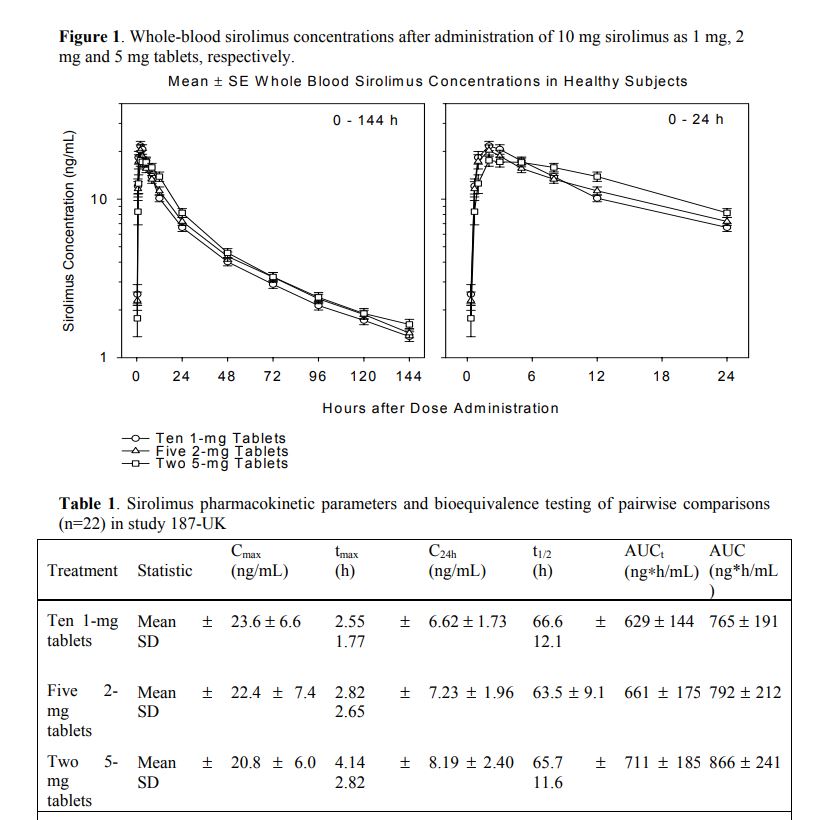
Time-to-peak (Tmax) also depends on whether you’re taking 1 mg, 2 mg, or 5 mg tablets of sirolimus.
3 Likes
Good to know! Would be really helpful see Cmax and time variables for capsules vs tablets. I’d expect capsules to be absorbed much faster and possibly higher Cmax, unless the powder being released in the stomach interferes significantly with absorption.
Incidentally, IF it’s true that stomach acid interferes w/absorption of rapa (can’t remember where I saw this?), I wonder how much it might increase absorption to take an H2 blocker such as famotidine before one’s weekly dose?
2 Likes
EnrQay, in the study you referenced, the study participants were given an oral solution containing 5 mg/mL sirolimus. In the other study I cited in this thread, the time-to-peak plasma concentration is significantly longer when taking sirolimus tablets.
1 Like
I’ll have a look, thanks!
1 Like
Most studies show significant inter individual pharmakinetics within the cohort. So unless we’re doing well controlled dosing protocols AND in parallel blood Sirolimus testing, most of us are flying blind. From what I can survey from various forums, very few people are doing this clinical grade-like monitoring. Side effects might serve as crude upper dosing limit cutoff, but is it the Cmax and/or AUC that is responsible? And what about measuring other biomarkers that are associated with Sirolimus…kidney and liver function, lipids, glucose, CBC? Other proxy markers? I’ve started to do some of this testing, but plan to bring more detailed monitoring this coming year.
3 Likes
I got the results for my second sirolimus test from Labcorp (ordered through Life Extension). My previous result measured the trough (see my Mar 3 post above) at <0.5ng/ml 7days after 3mg rapa with earlier grapefruit and fatty snack at the same time as rapa.
This test was 1.75 hours after my weekly 5mg, which was taken with a fatty snack, and taken about 2.5 hours after eating 8 oz whole grapefruit. Some might interpret this as excessive rapamycin, since the GF might multiply the effect by 3 - 3.5x and the fatty snack might increase absorption by 1/3.
My results: 17ng/mL, which seems right in the therapeutic range. Have others here posted results? I plan to get tested again in a couple of months to test my trough at this higher 5mg dose.
Any comments? Too high? Not high enough? It seems in line, maybe on the low side, with the graph at the top of this page.

2 Likes
Thanks for posting, this is amazing! Well done experiment.
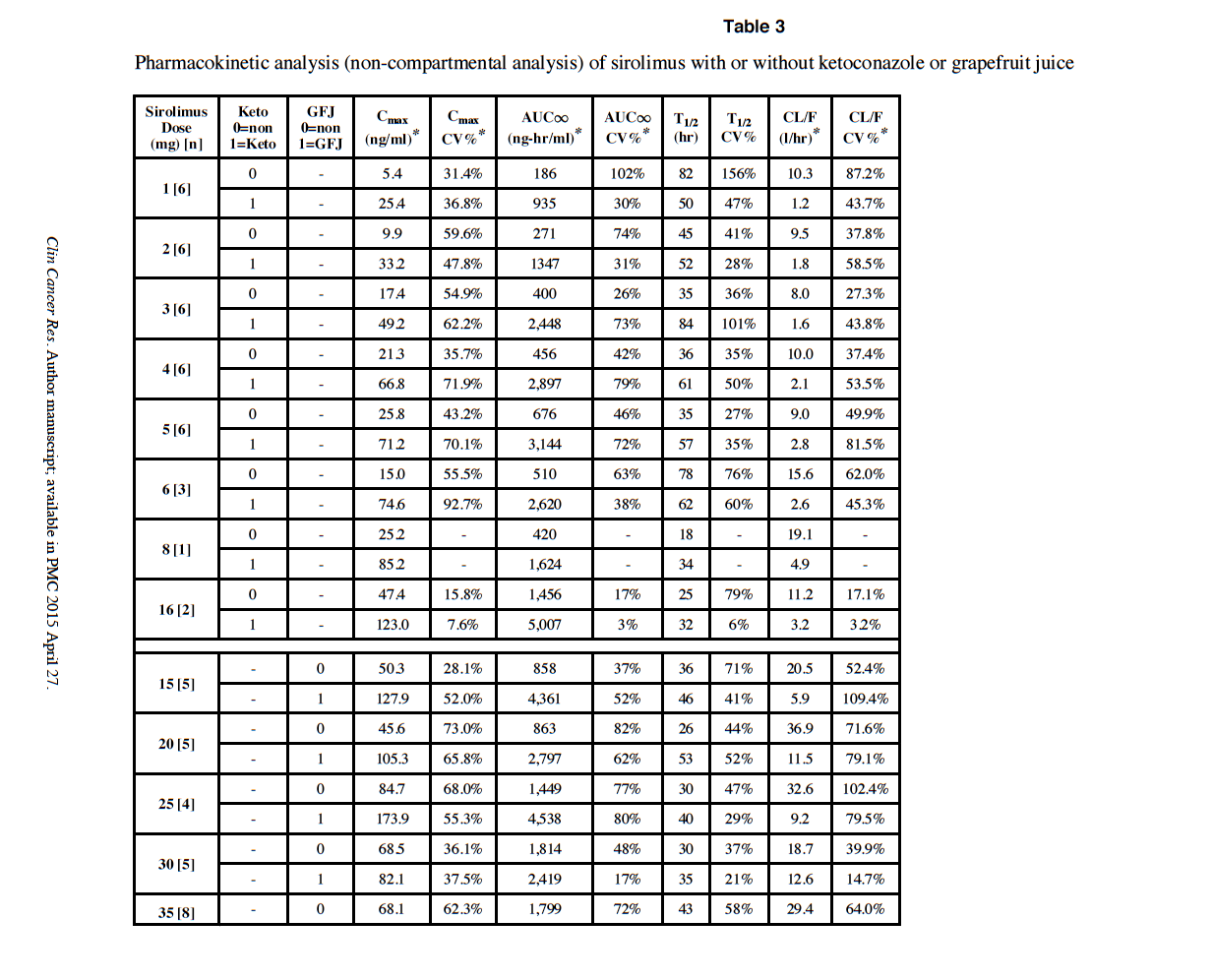
As for your Cmax with GFJ, it would appear to be low, based on this seminal paper on GFJ/Rapamycin pharmacokinetics.
“For the sirolimus plus grapefruit juice study, sirolimus was administered alone in week 1 and with grapefruit juice starting in week 2, one day prior to sirolimus. Grapefruit juice (supplied by Florida Department of Citrus), 240 cc, was administered once daily without interruption. This dosing was based on research demonstrating that the half-life of intestinal enzyme inhibition of grapefruit juice is 12 hours(21) thus providing time for modulation prior to sirolimus dosing”
At 5mg with GFJ, Cmax in the study is around 70 ng/ml. As you can see, there are some Cmax over 100 ng/ml.
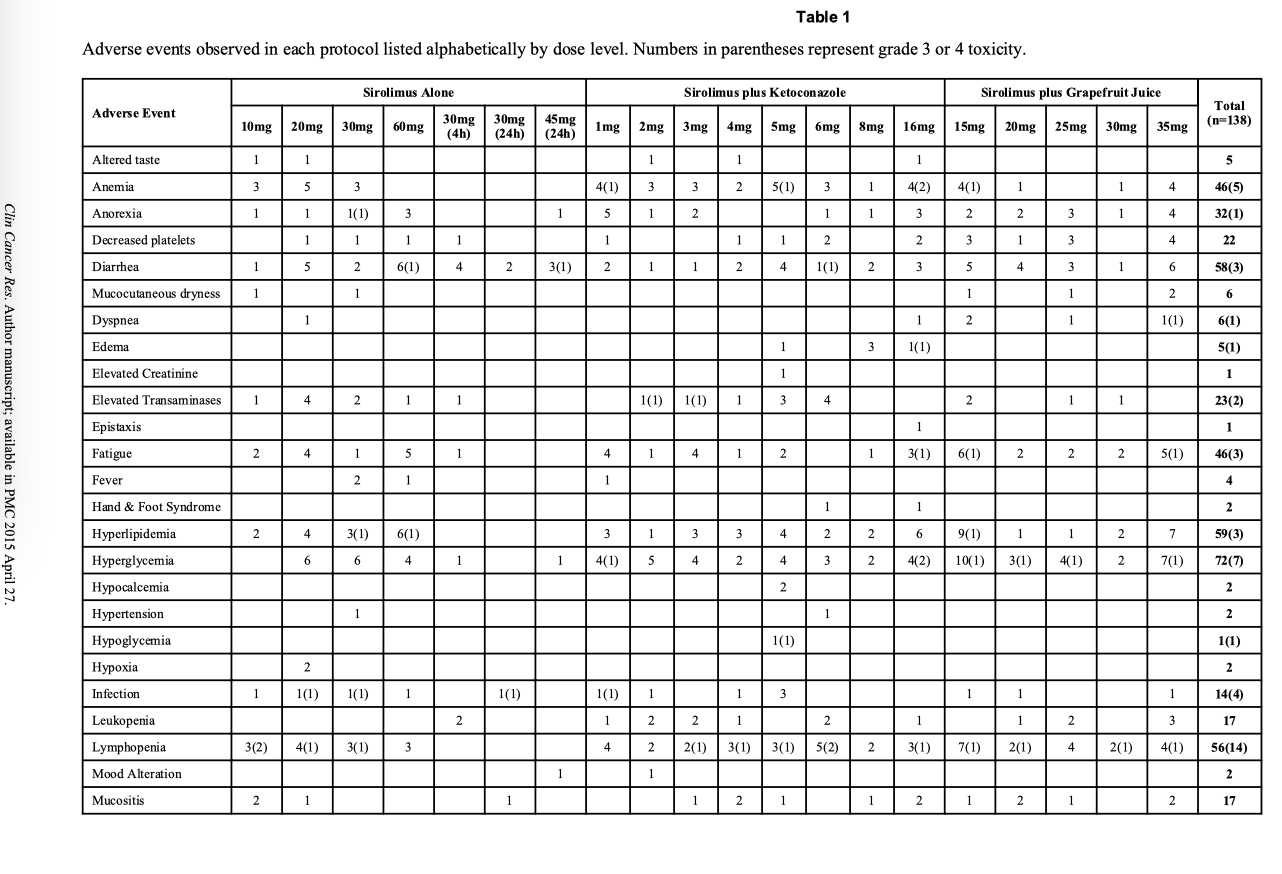
It’s the wild wild west for exploring the max without side effects. See Table 1 in the referenced study.
Yes, would be good to also get a trough measurement.
I am taking 12mg weekly with dual night before/morning of GFJ. But I’ve not fully vetted my Rapamycin current vendor.
I just got my new Rapamycin order, sending out for confirmation lab analysis, and then will redo a blood Sirolimus experiment, both trough, and trying to capture the signal after GFJ/dose. Will post.
3 Likes
If I am reading this chart right, 5mg rapa + ketoconazole produced Cmax=71.2. The grapefruit was tested only with 15mg-35mg levels. The 15mg +GF produced Cmax = 127.9. My own 5mg + GF produced Cmax=17. So, yes, if you scale down their 15mg to my 5mg, my Cmax seems low.
But the question remains, is this a good therapeutic range?
Yes - we really have very little idea here (at least in any specific, measurable way). Nor do we know how large the dose / response variation might be between people. Its frustrating to have so many unknowns around rapamycin.
1 Like
You are correct, I grabbed the wrong row.
Define “therapeutic”? I am 57, I doubt any of these definitive answers will come in my lifetime.
My current n=1 philosophy is to push the outer range, without significant side effects or blood marker dysregulation, balanced against superior physical and cognitive capabilities.
I had one canker sore, and no noticeable side effects, or blood marker dysregulation as of yet.
Wild type mice only die of cancer…Rapamycin delays their death, but they still die of the same cancers.
How many people on this forum are doing advanced preventative cancer, CVD, or brain imaging scans as yet another reference marker?
But humans die of a great many other causes, CVD, cancer, neurodegenerative, diabetes and all the related organ complications.
With all my hacks, I am trying to address as many mortality pathways as possible…the goal should be to push out all cause mortality.
2 Likes
You are right: we are guessing at what dose will produce a blood level that we don’t have therapeutic standards for.
I probably will do the same, carefully over time.
As I wrote and posted in another thread.
1 Like
Thanks for sharing, EnrQay.
Assuming you’re taking Sirolimus tablets, your peak level blood draw may have been performed a couple hours early (see my previous post above), so your true peak level may in fact be higher than the result you got.
From the FDA drug insert for Rapamune tablets:
“After administration of Rapamune Tablets and a high-fat meal in 24 healthy volunteers, Cmax, tmax, and AUC showed increases of 65%, 32%, and 23%, respectively.”
1 Like
Did anyone here attend the discussion with Matt Kaeberlein last week on the study, and was there any discussion around what we think we should be optimizing for in terms of dosing - Cmax, tmax, or AUC?
2 Likes
I think this is completely the right approach - we just need to be watching our bloodwork regularly (with a cost of about $70 per cycle its reasonable to do it every few months), and if things are fine there, and no bothersome side effects otherwise, slowly step it up.
I’ve found rapamycin to be surprisingly side effect free overall - I’ve taken doses as high as mid 30mg and really had no noticeable side effects (but need to track the blood work more closely).
3 Likes
Yes, I would love to hear Matt Kaeberlein’s thoughts on this topic.
In the ITP for the 42 PPM dose of sirolimus, male mice sirolimus blood concentration was 23 ng/mL (23% median lifespan extension, 8% max) & for females 80 ng/mL (26% median lifespan, 11% max)
1 Like
Given that our personal weights are all different, I wonder if it might be helpful to also share our dosing protocols expressed as milligrams of sirolimus per kilogram (mg/kg).
3 Likes
Yes (I’m at 0.07mg/kg/wk), and why is dosing of drugs sometimes expressed as mg/m^2 of surface area?
Rapamycin was approved in 2006, and has been used safely for almost 20 yrs. There is even a small study paper on “acute Sirolimus overdose” cases, all without any serious permanent effects.
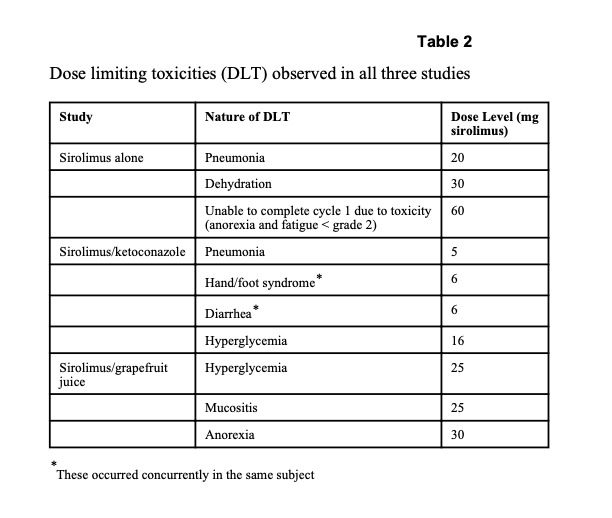
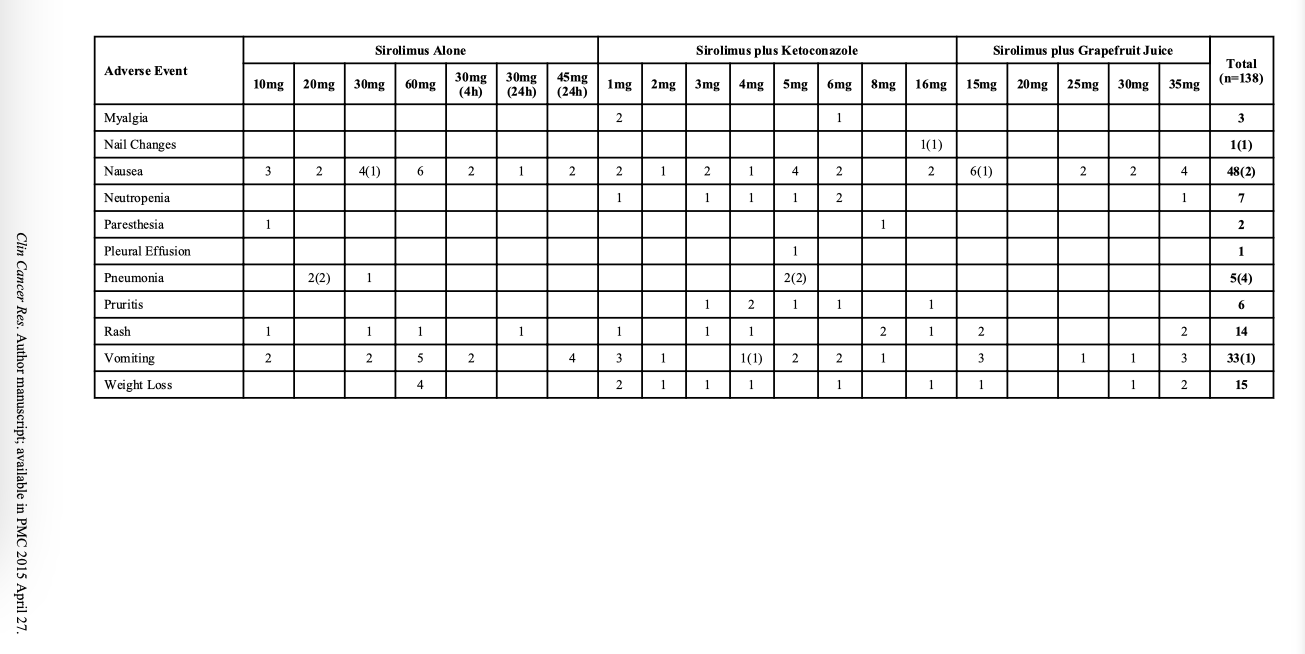
If we look at the GFJ/Ketoconazole/Rapamycin study side effects, in the Sirolimus alone or Sirolimus/GFJ combination, the DLT (dose limiting toxicities) are 20mg+ MIN. Most all of us are taking MUCH less than 20 mg/week.
With regular tracking of biomarkers, I think it’s relatively safe (my personal opinion, I am NOT a doctor, this is NOT medical advice) to explore pushing the envelope of weekly dose, everyone an n=1. I am under the care of a doctor in my journey.
I’ve extracted the side effects tables from the paper.
2 Likes
I just finished the video and there was no discussion of blood levels of rapamycin.
2 Likes