Does anyone have info on combining rapamycin with a keto diet?
I have seen studies suggesting that a keto diet suppresses mTor, but I don’t know how good the studies are.
I’m wondering if the benefits of diet + rap are cumulative, or if one replaces the other.
For example, if I take rapamycin, should I not bother with keto? Or if I do keto, do I get no benefit from rapamycin because I’m already inhibiting mTor? Or do they do different things, and it would be good to do both?
Hi M! Welcome to the site. I’m neither an expert on keto or rapamycin and autophagy so I’ll just try to provide links to info that I think might help answer the question.
Just to step back for a second - one thing to think about is what are you trying to optimize for? What is the goal? In the past year or so I got much more into keto - partly for the ketosis and autophagy, but also partly for weight loss.
Keto might be good for weight loss, but - what I found that what really helped me for weight loss was the metformin and the canagliflozin. For each of those - in sequence - I quickly and easily lost about 10 to 15lbs during the first month or two of using the medication (the first 3 months for metformin, the first two weeks for canagliflozin). I have tried, with varying levels of effort, to lose 10 or 15 lbs extra I was carrying for the past decade or more… and it never happened. It was really hard and frustrating. But it was really easy (for me at least) with metformin and then canagliflozin. And - its been really easy to keep it off too.
There is research that suggests that rapamycin use can help reset your weight “set point” to the new lower weight so you don’t tend to creep back up to your former weight. That has certainly been the case with me. Previously when I lost weight it always seemed to be hard, and then it also came right back in the months following the loss. With rapamycin and my weight loss this time - there has been no trend like before. The weight stays off, I’m not hungry , and I don’t gain the weight back. Its great.
Here is some of that research, but also anecdotally many people talk about how easy it is to lose weight on rapamycin and keep it off (note, but its not a weight loss drug - with just rapamycin you aren’t likely to lose much weight):
Of course you’ve also probably heard of the amazing success people are having with semaglutide and other GLP-1 drugs. I’ve heard of 20%+ weight loss in the first 6 months… Many people are also speculating that this type of drug would also offer lifespan enhancement for the average person.
My only point here is that if you’re primarily looking at keto for weight loss - there may be easier approaches. And, they can be done in concert with ketosis and rapamycin.
Right now keto is quite popular in the Rapamycin-using community - primarily, I suspect, because two well known rapamycin users (Peter Attia and Mikhail Blagosklonny) are both advocates of rapamycin and the keto diet.
Rapamycin and ketosis can, I’ve seen research suggesting, at least partly drive mTOR inhibition and thereby help induce autophagy in the body, which is one way both these techniques are theorized to help improve longevity.
You asked about whether the benefits of keto + rap are cumulative or do they replace one another - and I think the answer is nobody really knows for sure.
There is no way currently in the clinic or in the lab to measure autophagy. How much autophagy, in what cell types, etc. for a given dose of rapamycin, or ketosis (or fasting) really isn’t known from what I could determine. There is a new research that says they have identified a way to measure autophagy - but it hasn’t yet been translated into anything people can access or have used to start establishing benchmarks to answer the type of questions you’re asking - which effectively what is the dose/response relationship between things like rapamycin, keto, fasting, etc - and autophagy.
Here is that recent research on measuring autophagy:
and
Generally - it seems that Attia and Blagosklonny are tending to practice keto all the time, and layering on the rapamycin too.
With regard to the specifics of MTOR inhibition of keto vs. Rapamycin - I haven’t seen any great discussions or research on this - perhaps others here can add something I have missed.
Some other considerations are what type of Keto are you thinking of doing. I already have high cholesterol - so the traditional keto of eating tons of red meat, bacon, eggs, etc. was not a good option for me. At some point I heard about “Clean Keto” and decided that it was the better option for me - I encourage you to read up on it if you haven’t yet:
Lastly - I think some good resources on keto might be the following:
Anyway - perhaps this is the start of an answer to your question - and hopefully someone with more knowledge than I can jump in with more…
My main interest is increasing healthspan, particularly mental sharpness since I cared for a relative with Alzheimer’s.
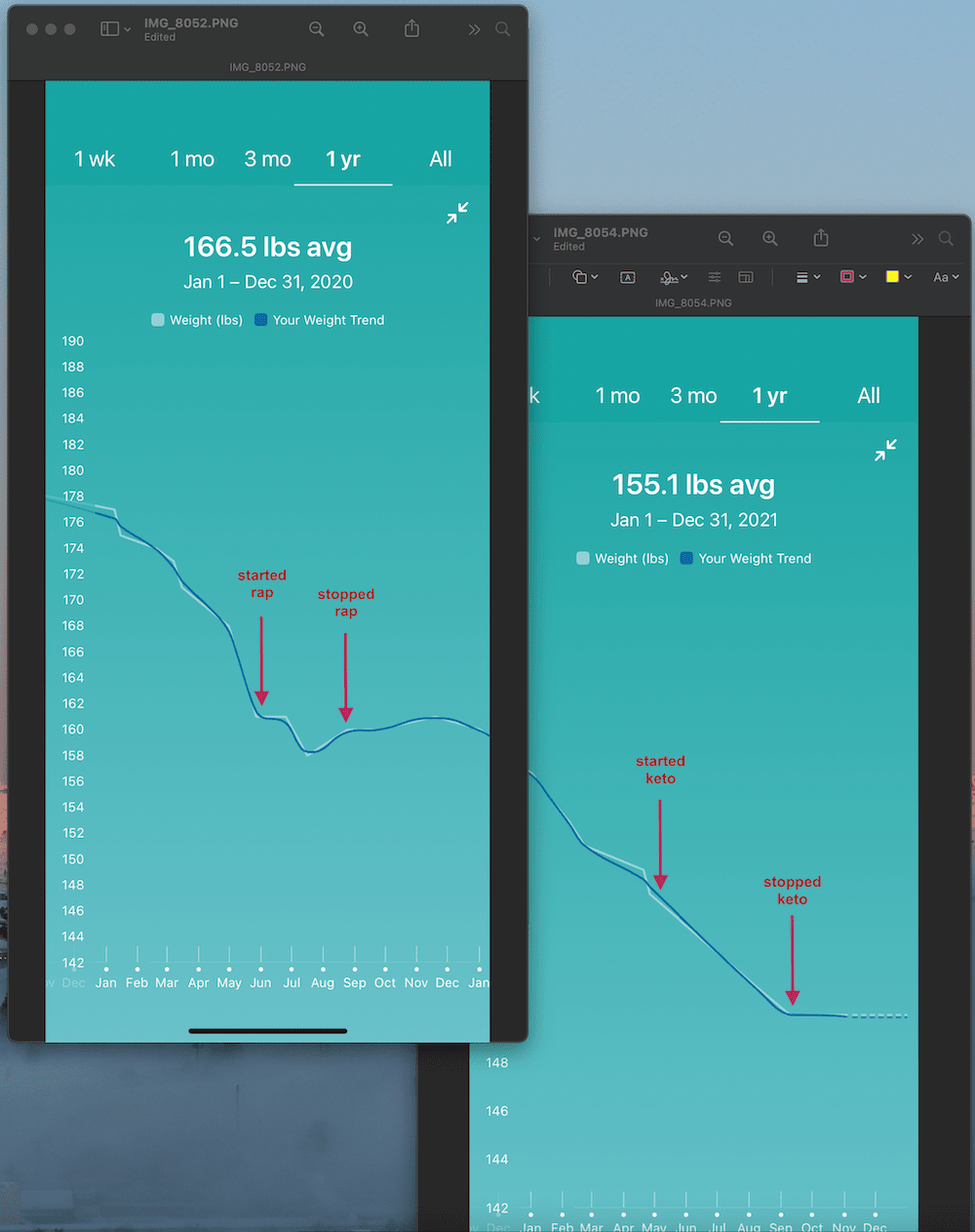
My sense was that rapamycin didn’t help me lose weight but that it did seem to help me keep it off. And my sense was that keto only mildly helped me lose weight. But then I realized I have data!
My activity level has been steady the whole time, and I wasn’t consciously restricting calories or actively trying to lose weight.
It’s important to note that the scale on these two graphs is different because I lost 18 pounds in 2020 and have only lost 11 so far in 2021, so lining them up like I did is a bit misleading.
The pandemic has been bad for a lot of things, but it has been great for me for weight loss in general because I used to eat in restaurants almost every day, and instead, I’ve been forced to cook. So it seems that just completely avoiding restaurant food had more of an effect than rapamycin or keto. I’ll never go back to my restaurant habit!
I just started rap again, and I think I’ll probably go back to keto in a month or two, so it will be interesting to see what happens with my weight.
Interesting that you mention mental sharpness and rapamycin.
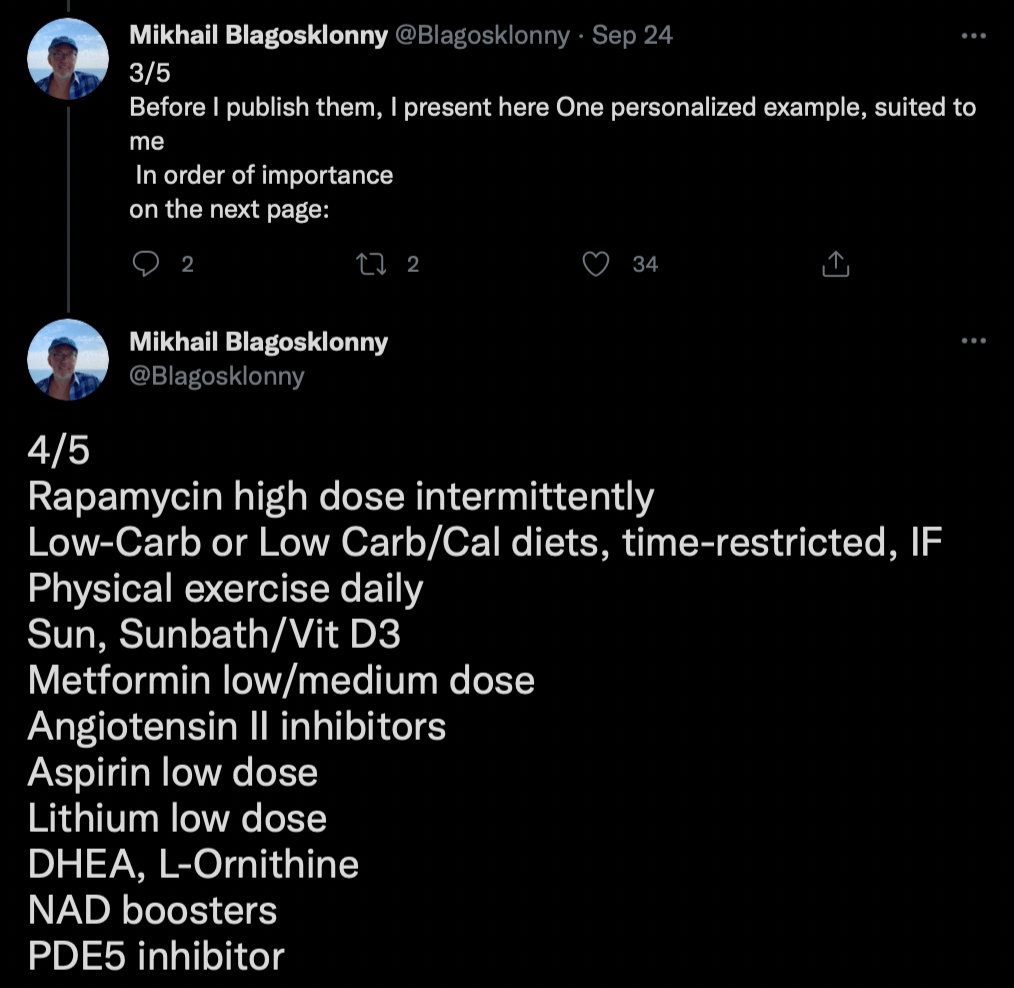
One of the key proponents of rapamycin - Mikhail Blagosklonny - has, in the past few months, modified his rapamycin regimen to be 20mg taken once every two weeks. He says he’s done this because he believes that rapamycin will, via this higher initial dose, be better at penetrating the blood brain barrier (and therefore help prevent brain aging).
See this post on rapamycin dosing protocols - mid way down:
But, I’ve never seen any data on this topic (I tried asking him on twitter, but no response)… so I’m not sure how valid this argument is.
You may want to do a little more research on this question - does a higher initial rapamycin dose penetrate the BBB better? Please let us know if you find anything.
Some papers that look relevant to the issue of brain health and rapamycin. I know that your background in science is far stronger than mine, so perhaps you can summarize or report back on anything interesting you discover in this information search of yours on this topic:
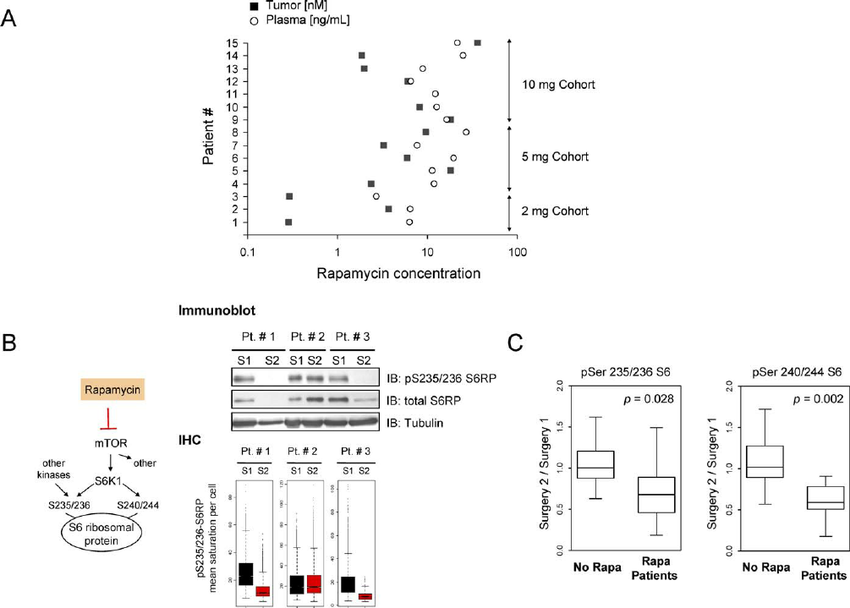
Rapamycin Crosses the Blood–Brain Barrier and Blocks mTOR in Tumor Tissue (A) Rapamycin concentrations in tumor tissue (filled squares) and peripheral blood (empty circles) grouped by rapamycin dose cohorts (2 mg, 5 mg, or 10 mg per os daily)
Thanks! Interesting stuff. I’ll keep an eye on the increased-dose-blood-brain-barrier idea.
If I remember correctly, Mikhail Blagosklonny said something similar in this recent video. I believe he said something like the best dose in his opinion is higher than what other people are currently doing. VitaDAO Discussion Panel - Rapamycin & Longevity - YouTube
The “Rapamycin and Alzheimer’s disease: Time for a clinical trial?” is the paper that pushed me over the edge to try it. I hadn’t seen the other one though, which also looks promising (with the caveat that it is an animal study).
Yes - the trend in people using higher doses of rapamycin has been accelerating the past year or so. The rationale by Blagosklonny and others is that in all the mice studies, the higher the dose (at least in male mice), the greater the longevity. As people have increasingly adopted rapamycin for anti-aging and since few people are reporting significant adverse events - the trend is to try higher doses.
Male mice lived 60% longer after the end of treatment, better muscle function, less cancer. The Female mice had no difference in lifespan, but they died with very different types of cancers (all had aggressive hematopoietic cancers compared to 30-40% in the rapamycin-treated [not uncommon for these mice to get this cancer]).
Basically - it seems like the researchers are working off the general theory that if we can find the highest dose of rapamycin possible - short of inhibiting mTORC2, that it is this dose that maximizes lifespan and healthspan.
It reminds me of this Jerry Seinfeld video / joke about the strength of medicines:
But of course - the closer you are getting to that imaginary “maximum dose” - the higher the risks… and it will likely vary between people a fair amount, so you don’t really know how much risk you’re taking… so there are some significant issues with this strategy.
I have a related question about Keto for you - since you are much more the scientist than I am.
Keto seems to lower MTOR which is good, and promotes lifespan.
But at the same time, many studies over the past 5 or so years have shown that protein restriction, and specifically methionine restriction, are both lifespan promoters.
So - how can the two above statements be true? And how does that impact your thinking about Keto?
Super interesting about the mouse high-dose studies.
For keto, people always think of it as being about protein, but in my understanding, it’s really all about fat. I actually had to limit my protein intake.
I was shooting for 70% of calories from fat, and it was really tough. I found that I mostly had to eat avocados, olives, olive oil, coconut, peanut butter, cheese, eggs, small amounts of nuts, and vegetables. Chicken breasts were completely out, for example, because they didn’t have enough fat and would supply too many calories from protein, meaning that I couldn’t get to 70% fat.
So for me, on a keto diet, I was very likely getting less protein than I would on a normal diet.
I’m not familiar with the methionine data, but looking at the first study, what jumps out at me is not the restricted protein but the high carbs. That is the opposite of what the keto studies say, so I can’t immediately say how to resolve those two different studies. I feel like I have seen quite a bit of data showing that people can “cure” their diabetes with a keto diet, and Dr. Bredesen (the author of “The End of Alzheimer’s”) has supposedly reversed dementia in a small number of Alzheimer’s patients with a complicated regimen, of which “healthy keto” is a part. (You’re also supposed to eliminate dairy, which in the end, I found too hard to stick with.)
I don’t know what to make of the high-carb diets in these papers. Bredesen does mention methionine restriction, so maybe the thinking is that with keto, you’re also getting protein restriction to levels that make a difference. But the high-carbs in those studies are in direct contradiction to everything else.
One of our other members here @Charles_Richardson has a lot of experience with Keto I know.
Charles - do you have any thoughts on @CuriousM questions above? (see top of the first posting - I should have pinged you earlier - but just remembered).
Well I’ve been doing keto off and on since the '60s. For me it’s the most effective weight loss diet. A couple of years ago, about the time I started rapamycin I lost 40 pounds doing pretty strict keto. Fish, meat, avocados, non-starchy vegetables, MCT oil and powder, heavy cream, red wine, basically.
And then up to my rapamycin to 6 mg a week or 9 mg a week and dropped 10 lb without even thinking about it or trying.
I’m convinced it does reset your set point because now I really can’t gain weight pretty much no matter what I do.
I think keto plus rapamycin is a good combo for a lot of people. But I also think everyone is different, and each person’s metabolism changes over time.
I’ve certainly seen the literature about methionine restriction and protein restriction but I just don’t know enough to make any intelligent comments about it. I’m not confident that anyone does.
I think rapamycin plus a low carb diet that’s also low in AGEs, along with regular exercise, and good sleep is going to get you 70 to 90% of what you can do longevity-wise for yourself at this point. Beyond that I really think it’s guess work. We don’t even really know what the optimum dosage or dosage schedule of rapamycin is.
Beyond those things it’s hard to imagine anything making a dramatic difference, well there are some molecules out there that seem to be helpful. And I imagine we will all continue to try them.
But if you don’t to those things I mentioned, all the various molecules and supplements aren’t going to make a significant difference.
One thing about keto that I think is important is not to make the mistake of adding extra fat just to add extra fat. But at the same time for a lot of people who have autoimmune diseases or conditions the higher the fat the better. So it just isn’t one size fits all.
The most important skill to learn is how to evaluate what a particular intervention does or doesn’t do for you.
I’m considering making turkey a go-to meat since it is unusually low in BCAAs, even compared to many plant sources. Since I get a moderate amount of protein overall (85g-ish g/day), I don’t think would exacerbate any sarcopenia problems.
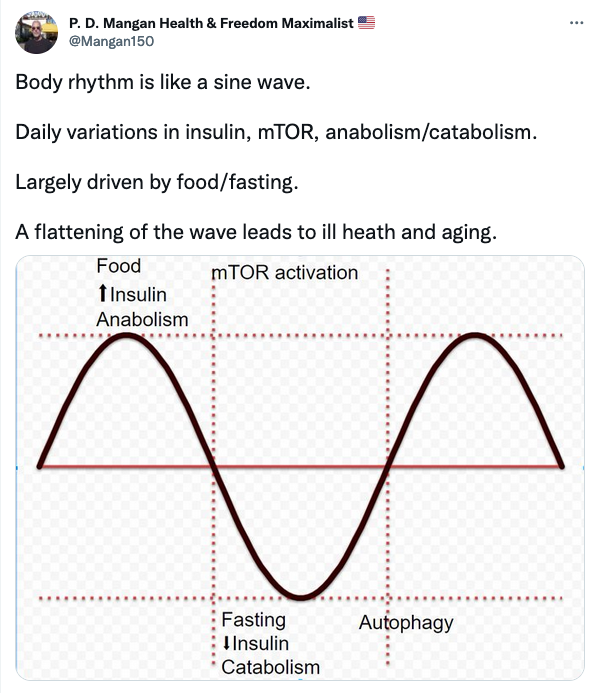
He goes on to say that: In aging and chronic disease, the sine wave is flatter. Preventing the sine wave from flattening can prevent chronic disease and slow aging.
It’s an analogy, rather than a study, so its accuracy is limited. However, we can imagine that in the case of chronic overeating, the sine wave would be flatter - and this would not be good. Similarly when people overeat glucose containing foods, the sine wave would be flatter, as insulin levels would stay elevated.
“We took a unique approach by targeting APOE4 because the usual drug targets, amyloid-beta and tau, have not produced a convincingly effective drug for people with AD despite decades of work,” said Johnson.
The researchers screened 595 compounds in a drug library from the National Institutes of Health and identified several compounds that specifically blocked the effect of APOE4 on Alzheimer amyloid formation.
“We then looked into the huge National Alzheimer’s Coordinating Center (NACC) database and asked what happened when someone was prescribed these drugs for normal indications but happened to be Alzheimer’s patients,” Potter said.
That’s when they found that psychiatric patients with AD using imipramine and olanzapine showed significant improvement in AD symptoms.
“The only things these drugs have in common is that they block the catalytic effect of APOE4 on the formation of amyloids in the brain,” Potter said, referring to the proteins that form clumps and disrupt cell function in AD.
The results were surprising.
“Our analyses show that, compared to the control populations, subjects taking imipramine or olanzapine had improved cognition and diagnoses, which are direct clinical measures of disease severity,” the study said. “Notably, in our drug screen, we found that imipramine and olanzapine strongly inhibited the apoE4-catalyzed fibrillization of Aβ (amyloid beta), whereas none of the other antidepressants or antipsychotics whose use was reported in the NACC database had any such activity and none showed any benefit for AD patients.”
The ketone bodies, especially β-hydroxybutyrate (β-HB), derive from fatty acid oxidation and alternatively serve as a fuel source for peripheral tissues including the brain, heart, and skeletal muscle. β-HB is currently considered not solely an energy substrate for maintaining metabolic homeostasis but also acts as a signaling molecule of modulating lipolysis, oxidative stress, and neuroprotection. Besides, it serves as an epigenetic regulator in terms of histone methylation, acetylation, β-hydroxybutyrylation to delay various age-related diseases. In addition, studies support endogenous β-HB administration or exogenous supplementation as effective strategies to induce a metabolic state of nutritional ketosis. The purpose of this review article is to provide an overview of β-HB metabolism and its relationship and application in age-related diseases. Future studies are needed to reveal whether β-HB has the potential to serve as adjunctive nutritional therapy for aging.
New information posted here often leads me down rabbit holes looking for related information.
Today the BHB post led me to HMB. I really don’t know how I missed this one. BTW, I was taking BHB when I was on a keto diet. It works quite well.
At this stage of my life, I like to experiment with new supplements that might preserve or enhance muscle mass. HMB looks to be promising even for those who don’t exercise.
“Conclusion: Our findings suggest that HMB has a positive effect on body composition and strength, especially in bedridden or sedentary elderly, due to its anticatabolic properties.”
“Supplemental HMB has been used in clinical trials as a treatment for preserving lean body mass in muscle wasting conditions, particularly sarcopenia, and has been studied in clinical trials as an adjunct therapy in conjunction with resistance exercise.[11][16][30] Based upon two medical reviews and a meta-analysis of seven randomized controlled trials, HMB supplementation can preserve or increase lean muscle mass and muscle strength in sarcopenic older adults.”
“The essential amino acid leucine and its metabolite β-hydroxy-β-methylbutyrate (HMB) have also received increased interest during recent years and are now widely used by sportsmen and bodybuilders as nutritional anabolic supplements. Both human and animal studies have shown effects on protein synthesis, muscle hypertrophy, decreased muscle damage and muscle soreness, modulation of the cholesterol profile and even improved emotional status”
And HMB is pretty cheap and doesn’t taste bad. I have been taking it for about a year. Not really sure if it does anything to be honest (unlike creatine, beta alanine and citrulline malate) but as I said it doesn’t taste bad and it’s generally regarded as safe even at high dosages