From my N=1, my insulin sensitivity is exceptional after 2 years of weekly use of at least 10 mg equivalent (3 mg + GFJ + EVOO). (sometimes at very high doses - 21 mg equivalent 7 mg + GFJ + EVOO)
My fasting insulin:
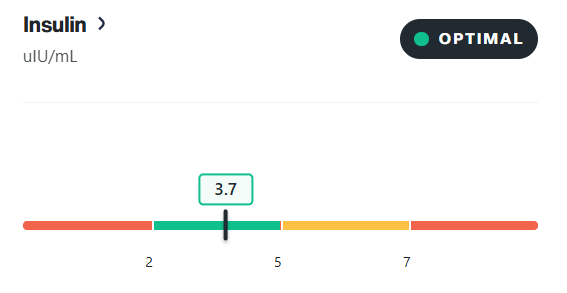
From my N=1, my insulin sensitivity is exceptional after 2 years of weekly use of at least 10 mg equivalent (3 mg + GFJ + EVOO). (sometimes at very high doses - 21 mg equivalent 7 mg + GFJ + EVOO)
My fasting insulin:
I had recent lab tests back and my A1C is down to 4.9 after it was 5.5 about 5 months ago. This is all while being on 5mg Rapamycin per week and lowering Rosuvastatin from 5mg to 2.5mg daily. 3mg Retatrutide, 10mg Empagliflozin, and 200mg Acarbose are the drugs I am taking to lower it.
So basically, my Rapamycin use is being offset as far as insulin resistance goes.
GLP1 agonists are very powerful insulin sensitizers so Reta alone could probably account for it.
Bingo. Since I was already on the other things before so all I did was cut rosuvastatin in half to 2.5mg and continue Reta (3mg per week divided MWF).
My A1C 5.5 bothers me, but iam resistant to take Reta. Iam very slim(BMI 20,6)…
I posted this elsewhere a while back but copying it here
I did a baseline IGF-1 prior to starting weekly Rapamycin. It was 74. After six months of weekly regimen, the IGF-1 went upto 115!
A1c(5.1), Lipids etc remain same. Omega index remains horribly low ( not that Rapa has anything to do with it; just my vegetarian diet). Can’t seem to figure out the IGF-1 trend though!
Yes, my testosterone levels did drop. Levels were drawn at the trough of Rapa. In other words immediately prior to weekly dosing.
Here is a link to the discussion of how IGF-1 and longevity have a U-curve association:
For people that use say daily sirolimus for organ transplant, Im guessing they need something strong like pioglitazone to control insulin resistance. For weekly dose it shouldnt affect much but if it does adding an extra day between dosing (once every 8 days instead of 7) might be all that is needed
My IGF-1 is high as well, although I never attributed it to Rapamycin. I would assume that Rapamycin would counter any negatives from high IGF-1 through MTOR1 inhibition.
Has anyone on CGM tried Allulose?
Metabolic Link Podcast – Allulose Episode (2024 Metabolic Health Summit Panel)
I. Show Introduction
Host: Dom D’Agostino, Ph.D.
Theme: Metabolism as the common thread in health & disease.
II. Episode Focus: Allulose
Rare release of full 2024 Summit panel discussion.
Goal: translate latest science → real-world metabolic-health tools.
III. Expert Panel
Richard Johnson, MD – Professor of Medicine, Univ. Colorado.
Jeff Volek, Ph.D., RD – Professor Human Sciences, Ohio State.
Ben Bikman, Ph.D. – Professor Cell Biology, BYU.
Andrew Koutnik, Ph.D. – Research Scientist, Samson Diabetes Research Institute.
Dominic D’Agostino, Ph.D. – Assoc. Prof. Pharmacology & Physiology, Univ. South Florida.
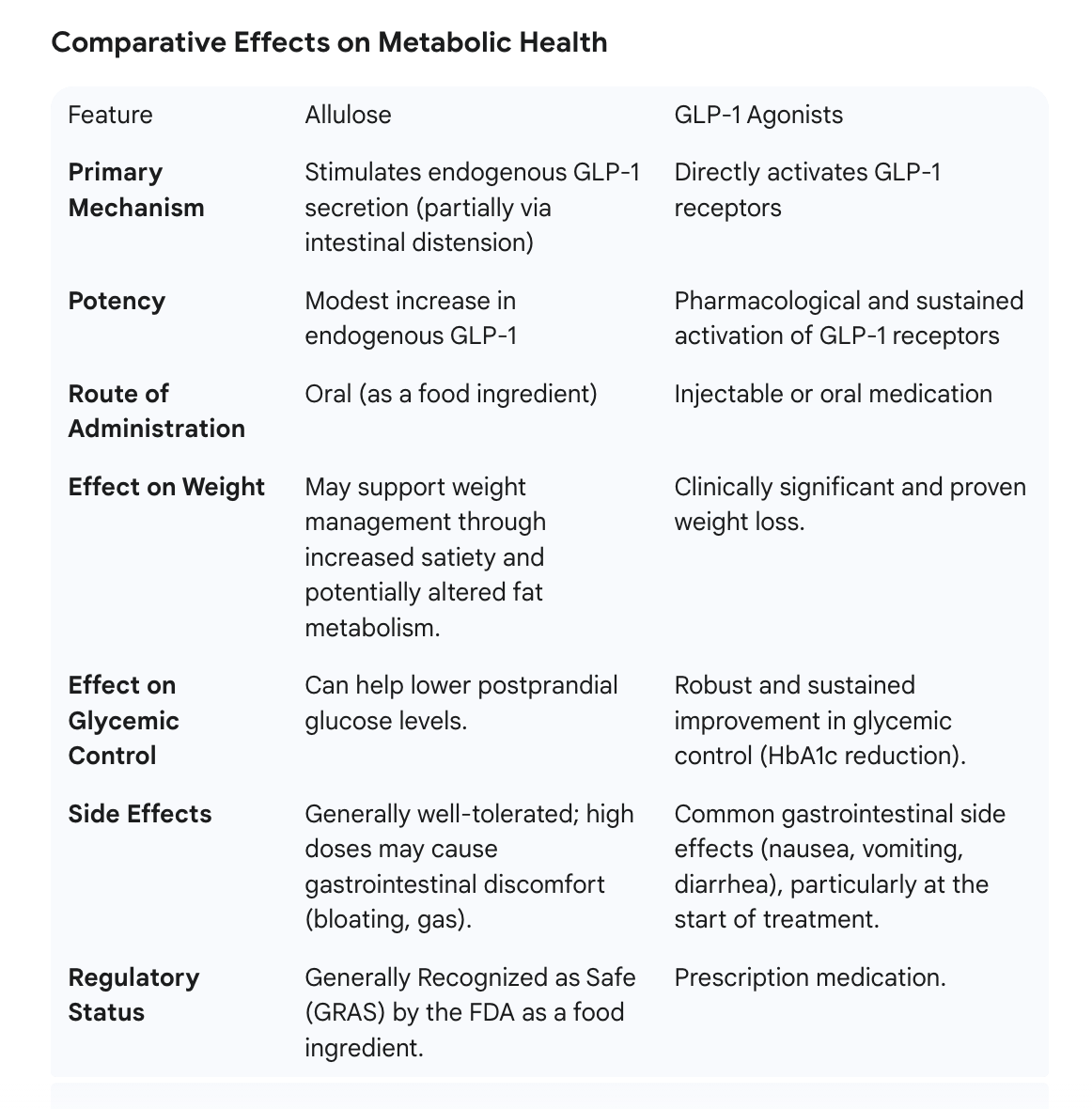
IV. Key Science Points Discussed
Glycemic impact: 0-5 g allulose blunts post-prandial glucose & insulin excursions.
Insulin sensitivity: acute & chronic improvements in clamp & CGM studies.
Weight management: ↓ energy intake via early satiety signals; animal data show ↓ fat mass.
GLP-1 pathway: dose-dependent secretion → delayed gastric emptying, enhanced insulin release.
Fructose comparison: minimal hepatic metabolism → low uric-acid & lipogenesis risk.
Safety profile: FDA GRAS; ≤ 0.66 g/kg/day GI tolerance in adults.
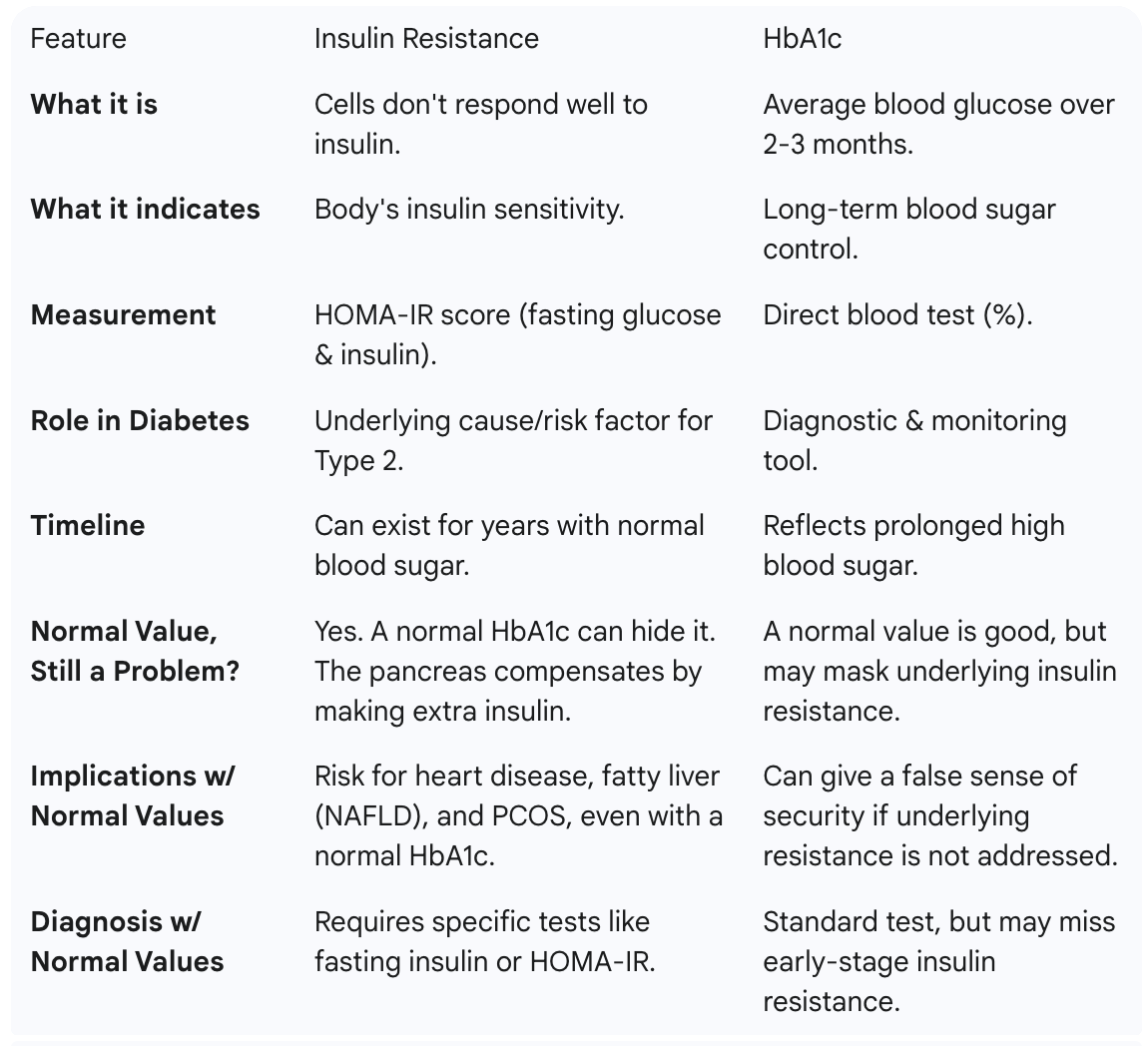
A normal HbA1c is a positive indicator, but it does not rule out the presence of insulin resistance.
Yes, and it doesn’t spike blood glucose. In my readings, it often decreased glucose levels. It’s my sugar additive of choice.
I use glycine whenever I need to add sugar. It also provides a longevity boost in addition to making your drink sweet! Win-win.
I agree. Glycine is naturally sweet. I add it to my cacao drinkr, morning coffee. I have used Allulose if and when Ican buy it on discounted price.
I am looking for a microdosing GLP-1 alternative, given that I am not qualified for the prescription.
I generally use sucralose but want to lessen the amount I take in as I use it in my coffee and my protein powder is sweetened with it. I don’t mind the taste and it doesn’t upset my GI. However I have to limit the amount of allulose or taglatose I take in or I predictably get GI upset.
Do the GI effects of these other sweeteners go away with continued consistent use or do others have the same issues?
I would look for a different protein powder.
Per the OpenEvidence.com AI
“Sucralose use is associated with increased risk of adverse metabolic and cardiovascular outcomes, including insulin resistance and coronary heart disease, and its long-term safety remains under active investigation.”
Artificial Sweeteners and Risk of Cardiovascular Diseases: Results From the Prospective NutriNet-Santé Cohort.
Debras C, Chazelas E, Sellem L, et al.
BMJ (Clinical Research Ed.). 2022;378:e071204. doi:10.1136/bmj-2022-071204.
Nonnutritive Sweeteners and Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Prospective Cohort Studies.
Azad MB, Abou-Setta AM, Chauhan BF, et al.
CMAJ : Canadian Medical Association Journal = Journal De l’Association Medicale Canadienne. 2017;189(28):E929-E939. doi:10.1503/cmaj.161390.
New podcast: You can have normal glucose and still have insulin resistance.
Sign of insulin resistance: skin tags, especially in the neck area, dry skin, and lower pulse pressure > 40

Remind us what are your stacks and what is HbA1C?
My HBA1C is a littl high at 5.6 but on a downwards trend.
My stack is found here:
Thanks! What do you think of the comments from AI: * Zinc 50 mg daily (or even 3× wk) can push copper low → consider 2 mg copper every other day if you stay on that dose.
Mag-citrate 210 mg gives only ~60 mg elemental Mg – low if you’re aiming for 400-500 mg/d; you get more from diet or add a second cap.
Lithium orotate 5 mg elemental is micro-dose, but still check 6-monthly eGFR if you keep it long-term.
Creatine + empagliflozin: both can nudge creatinine up – monitor eGFR; stay hydrated.
NAC 2 g is fine, but stop 48 h before any elective surgery (bleeding risk).
1. LONGEVITY / mTOR–AMPK–AUTOPHAGY
Rapamycin 3 mg w/ GFJ + EVOO – once weekly
Metformin XR 500 mg at night
Empagliflozin 12.5 mg morning
2. LIPIDS / CV
Atorvastatin 5 mg at night
Telmisartan 20-40 mg morning – STOPPED (low BP)
3. HORMONE / PROSTATE / HAIR
Dutasteride 0.5 mg at night
Horbaach Prostate Support (dose per cap)
Zinc 50 mg Mon-Wed-Fri
4. COGNITION / NEURO
Galantamine 4 mg at night
Lithium orotate 5 mg Mon & Thu
NMN 1 g morning
CoQ10 100 mg Mon-Wed-Fri
Coffee 1 & 2 (4 cups total)
Decaf chamomile/berry tea night
5. JOINTS / SKIN / GUT
Collagen peptides 11 g
Hyaluronic acid 500 mg
Glycine 5 g morning + 5 g night
Turmeric + black pepper
Magnesium citrate 210 mg
Brillo EZ 1 tab night
6. PERFORMANCE / BODY-COMP
Creatine monohydrate 5 g
Taurine 6 g
Citrulline 2 g
Whey 25 g (switching to plant)
7. MICRONUTRIENTS / ANTIOXIDANTS
Vitamin D3 5 000–10 000 IU morning
Vitamin B12 2 000 mcg morning
Super B-Complex Mon & Thu
NAC 2 g
Lutein 20 mg + Zeaxanthin 4 mg