Oxford and Nottingham researchers show that low-dose rapamycin protects aging human immune cells by directly reducing DNA damage itself, a mechanism separate from its known effects on metabolism, autophagy, or cell division, and confirm the effect in a small human trial.
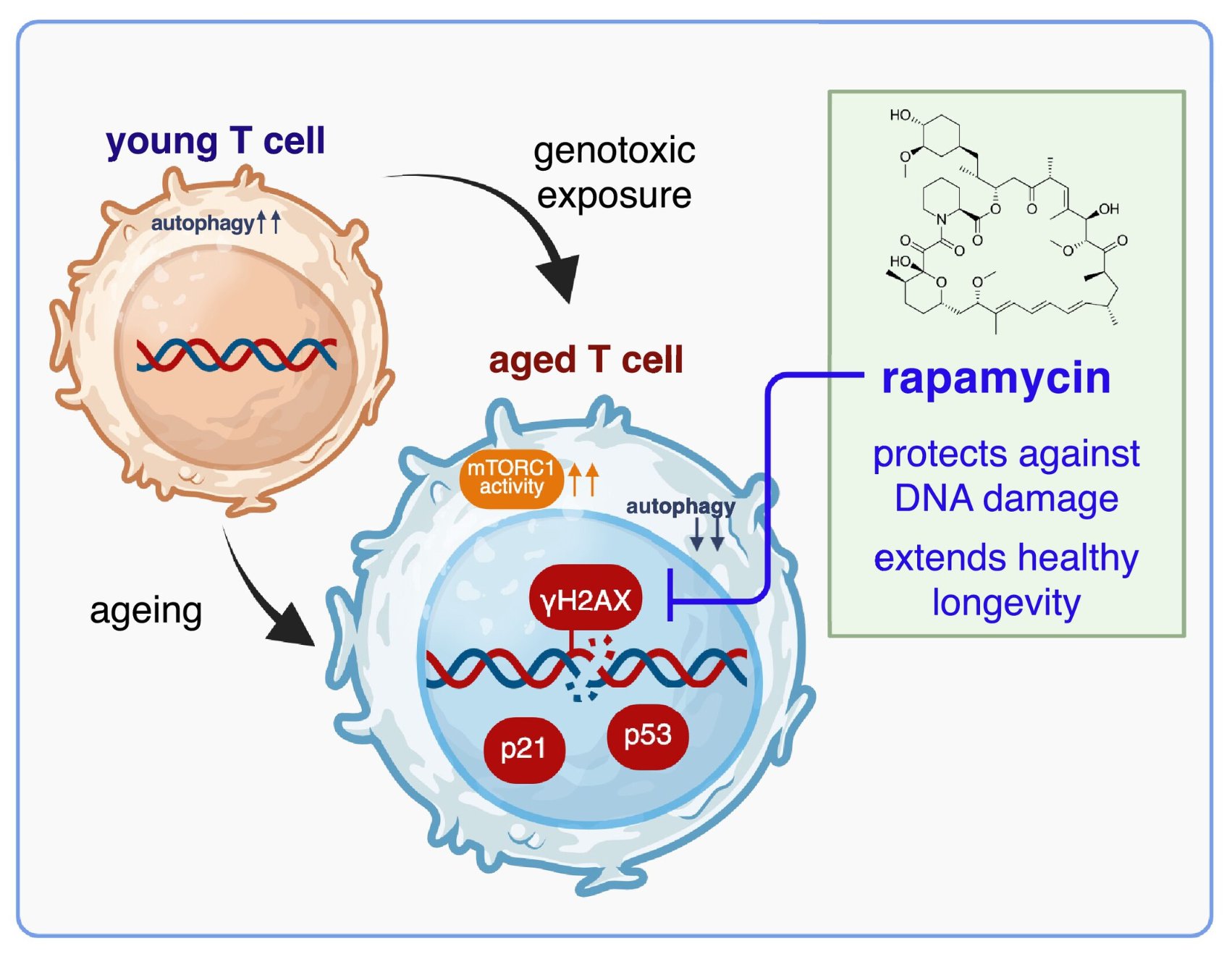
For fifteen years, rapamycin has been the closest thing longevity science has to a sure bet: it extends lifespan in every species tested, from yeast to mice, to monkeys. But nobody could fully explain why. The textbook story was indirect: rapamycin dials down the mTOR growth engine, slowing protein manufacturing, quieting cell division, and switching on autophagy, the cell’s recycling system. This new work argues those explanations miss the headline act.
The team, led by Loren Kell with senior scientists Ghada Alsaleh, Lynne Cox, and Katja Simon, went hunting for the source of rapamycin’s power in the immune system, the tissue whose decline arguably drags the rest of the body into old age with it. They deliberately blasted human T cells with zeocin, a chemical that shreds DNA into double-strand breaks, then watched what rapamycin did.
The result was striking. Rapamycin didn’t just clean up damaged cells after the fact; it reduced the actual burden of DNA lesions, measured by the “comet assay,” which physically visualizes broken DNA trailing out of a cell like a tail. Cells given rapamycin carried far less damage, and crucially, they survived. In untreated cultures, the genotoxic hit killed roughly 80 percent of T cells within 24 hours. With rapamycin, around 60 percent were still alive, a threefold survival advantage.
The protection was oddly forgiving of timing. Whether rapamycin was added before, during, or after the DNA-damaging insult, the cells fared better. And the team methodically ruled out the usual suspects: the benefit did not depend on slowing protein synthesis, halting the cell cycle, or boosting autophagy. Something more direct was happening at the level of the genome.
They then profiled immune cells from older people using high-dimensional cytometry, finding that aged immune subsets are enriched for markers of DNA damage, senescence, and mTOR hyperactivity, especially the DNA-damage protein p21. Finally, in a small placebo-controlled human trial, four months of 1 mg/day rapamycin significantly lowered p21 across most immune subsets versus placebo.
The big idea: rapamycin may be a genuine “genoprotector.” If it can shield DNA in a 70-year-old’s immune cells, its potential stretches beyond healthy aging toward cancer radiotherapy recovery and even radiation exposure during spaceflight.
Actionable Insights
The practical signal here is narrow but real, and it directly concerns anyone already microdosing rapamycin for longevity.
Dose and exposure. The human arm used 1 mg/day, producing a mean steady-state blood trough of roughly 3.24 nM, within the same order of magnitude as the 10 nM used in cell culture. Critically, at this dose there was no leukocyte suppression, addressing the perennial fear that rapamycin blunts immunity. This supports the “low-dose, non-immunosuppressive” microdosing philosophy rather than weekly high-dose pulsing for this particular endpoint.
Effect magnitude. The most quantifiable benefit is cellular survival under genotoxic stress: death fell from ~80% to ~40% at 24 hours, an absolute risk reduction of ~40 percentage points and a relative risk of death of ~0.5 (a 50% reduction). Framed as survival, that is a 3-fold improvement. The DNA-lesion reduction (comet Olive moment) was highly significant (p<0.0001) and appeared within 4 hours, even at the 0-hour timepoint.
Take-home. The in-human evidence is limited to a biomarker (p21 reduction), not a clinical outcome. For existing rapamycin users, it strengthens the mechanistic rationale that low-dose rapamycin plausibly defends genome integrity in the immune compartment. It also raises a genuinely novel, testable idea: short-course rapamycin around radiation exposure (medical or occupational).
Full paper: https://www.biorxiv.org/content/10.1101/2025.08.15.670559v1
Context / Source
- Full title: “Rapamycin Exerts Its Geroprotective Effects in the Ageing Human Immune System by Enhancing Resilience Against DNA Damage.”
- Access: Open access (CC-BY 4.0), both as bioRxiv preprint and published article.
- Institutions: University of Oxford (Biochemistry; NDORMS; Kennedy Institute) and University of Nottingham (COMAP/MRC-Versus Arthritis Centre), United Kingdom; with contributions from Ritsumeikan University (Japan) and the Max Delbrück Center (Germany).
- Publication status: Originally posted to bioRxiv (August 2025); received 25 September 2025, revised 19 December 2025, accepted 24 December 2025, now published in Aging Cell (2026, 25(2):e70364).
Summary
- Rapamycin, an mTOR inhibitor, is the most consistent lifespan-extending drugs in animals.
- At low (non-immunosuppressive) doses, rapamycin reduces cellular senescence but the underlying mechanism in humans was unclear.
- DNA damage is a major driver of immune ageing (immunosenescence), which accelerates whole-body ageing.
Main Findings
-
Rapamycin protects immune cells from DNA damage
- In human T cells exposed to genotoxic stress (zeocin, hydrogen peroxide), rapamycin reduced DNA damage markers (γH2AX, p53, p21) and improved cell survival.
- This protection was not due to slowing protein synthesis, halting the cell cycle, or increasing autophagy.
- Instead, rapamycin directly lowered the DNA lesion burden—showing a “genoprotective” effect.
-
Mechanism: direct genoprotection
- Rapamycin reduced DNA breaks (comet assay) and improved T cell viability after DNA damage.
- This effect was independent of classical pathways (autophagy, cell cycle arrest).
- Suggests rapamycin enhances genome stability itself.
-
Immune ageing is linked to DNA damage + mTOR hyperactivation
- Blood samples from older adults showed immune cell subsets (e.g., TEMRA T cells, B cells, monocytes) enriched for DNA damage and senescence markers (p21, p53, p16, γH2AX).
- These age-related cells also showed overactive mTOR signalling.
-
In vivo human trial (pilot study, NCT05414292)
- Older men (50–90 years) received 1 mg/day rapamycin or placebo for 4 months.
- Rapamycin significantly reduced p21 (DNA damage-induced senescence marker) in immune cells compared to placebo.
- Rapamycin also reduced immune exhaustion markers (KLRG1, LAG3, NKG2A) without immunosuppression.
- Blood levels of rapamycin were low but within the protective range.
Implications
-
Rapamycin acts as a genoprotector, a newly recognized mechanism that may explain its strong anti-ageing effects.
-
Potential applications:
- Healthy ageing: slowing immunosenescence.
- Medicine: protecting healthy cells from DNA damage during radiation/chemotherapy.
- Space travel: mitigating cosmic radiation damage.
- Pandemic preparedness: boosting immune resilience in older adults (e.g., against viruses that induce DNA damage).
![]() Bottom line:
Bottom line:
The study demonstrates for the first time that low-dose rapamycin directly protects human immune cells from DNA damage and reduces senescence in vivo, positioning it as a potential therapy to slow immune ageing and enhance resilience in contexts of DNA damage.