Researchers have long known that the mTOR inhibitor rapamycin is a potent life-extending compound across species, yet its precise mechanisms in humans remain somewhat elusive. A recent paper from the University of Oxford and collaborators, published in Aging Cell in the UK, shifts the paradigm on how this longevity drug operates. Rather than merely slowing cellular growth or boosting recycling pathways, low-dose rapamycin acts as a direct shield for the genome.
The study investigated human T cells exposed to genotoxic stress and found that rapamycin dramatically suppressed DNA damage-induced senescence. Critically, it did not achieve this by halting cell division, slowing protein synthesis, or upregulating autophagy—the traditional mechanistic suspects. Instead, it directly reduced the physical burden of DNA lesions and improved cellular survival rates following severe stress. Translating this to clinical relevance, the research team conducted a pilot placebo-controlled trial in older adults. Administering a low dose of 1 mg/day for four months, they observed a significant reduction in p21, a primary marker of cellular senescence, within the circulating immune cells of the treatment group. Exhaustion markers on T cells also dropped. This indicates that low-dose mTOR inhibition actively protects the human immune system from the DNA instability that drives age-related decline. For biohackers and clinicians focused on healthspan, this provides actionable evidence that rapamycin’s geroprotective effects translate to practical human immune resilience.
Rapamycin, an mTOR inhibitor, is the most consistent lifespan-extending drugs in animals.
At low (non-immunosuppressive) doses, rapamycin reduces cellular senescence but the underlying mechanism in humans was unclear.
DNA damage is a major driver of immune ageing (immunosenescence), which accelerates whole-body ageing.
Main Findings
Rapamycin protects immune cells from DNA damage
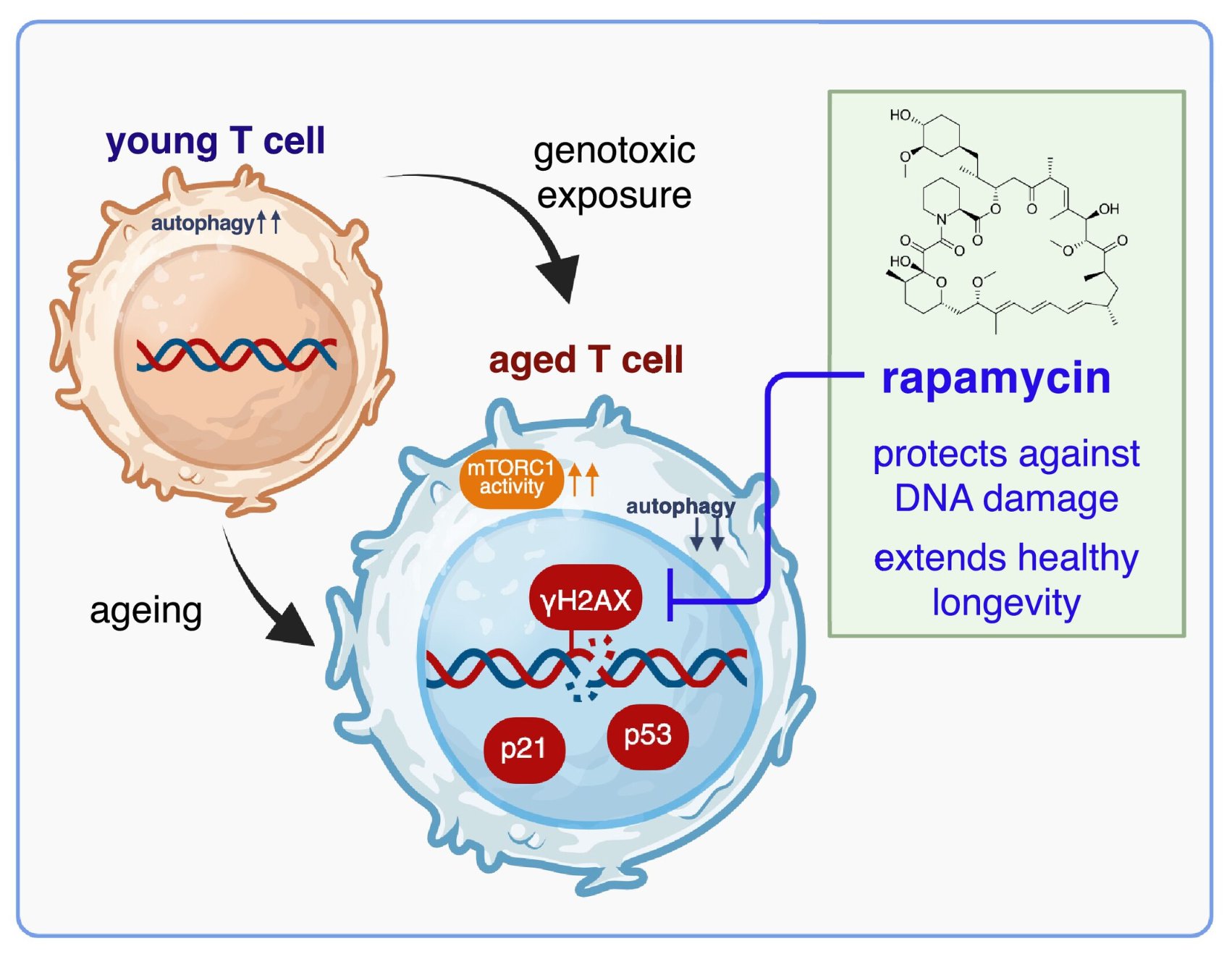
In human T cells exposed to genotoxic stress (zeocin, hydrogen peroxide), rapamycin reduced DNA damage markers (γH2AX, p53, p21) and improved cell survival.
This protection was not due to slowing protein synthesis, halting the cell cycle, or increasing autophagy.
Instead, rapamycin directly lowered the DNA lesion burden—showing a “genoprotective” effect.
Mechanism: direct genoprotection
Rapamycin reduced DNA breaks (comet assay) and improved T cell viability after DNA damage.
This effect was independent of classical pathways (autophagy, cell cycle arrest).
Immune ageing is linked to DNA damage + mTOR hyperactivation
Blood samples from older adults showed immune cell subsets (e.g., TEMRA T cells, B cells, monocytes) enriched for DNA damage and senescence markers (p21, p53, p16, γH2AX).
These age-related cells also showed overactive mTOR signalling.
In vivo human trial (pilot study, NCT05414292)
Older men (50–90 years) received 1 mg/day rapamycin or placebo for 4 months.
Rapamycin significantly reduced p21 (DNA damage-induced senescence marker) in immune cells compared to placebo.
Rapamycin also reduced immune exhaustion markers (KLRG1, LAG3, NKG2A) without immunosuppression.
Blood levels of rapamycin were low but within the protective range.
Implications
Rapamycin acts as a genoprotector, a newly recognized mechanism that may explain its strong anti-ageing effects.
Potential applications:
Healthy ageing: slowing immunosenescence.
Medicine: protecting healthy cells from DNA damage during radiation/chemotherapy.
Space travel: mitigating cosmic radiation damage.
Pandemic preparedness: boosting immune resilience in older adults (e.g., against viruses that induce DNA damage).
Bottom line:
The study demonstrates for the first time that low-dose rapamycin directly protects human immune cells from DNA damage and reduces senescence in vivo, positioning it as a potential therapy to slow immune ageing and enhance resilience in contexts of DNA damage.
Very cool! And I like that it was 4 months, which is a decent length of time. And 1mg/day, though not a “standard longevity” weekly dose, is not unreasonably high.
Sample size for the human volunteers was very low though (5 subjects per group)
1 mg / day for months was what was also shown to functionally render apoE4 brain similar to apoe3 so I’m seeing a lot of backing for this dosage — maybe with a washout period as a safety valve.
Also interesting that mechanistically they couldn’t attribute the effects to autophagy or any of the run of the mill mechanisms.
It’s interesting that the dose is 1mg/day. I have been on that dose for kidney transplant maintenance since 2010. No washout periods were recommended in my case. According to my experience it’s hard to be on this comparatively low dose for a long time bc of side effects.
I suppose no washout would be recommended in your case due to the primary reason for taking it being organ transplant so you can’t “afford” washout without bringing into the fold some other immunosuppressant.
May I ask 1) why was such a low dose recommended to you — it’s my understanding that for organ transplant the Sirolimus dosage employed is typically much higher 2) what were the side effects for you and how long did it take you to develop them on 1mg/day?
I do not know the reason why I was put on only 1 mg Rapa. Initially it was on combination with a low dose Tacrolimus which I couldn’t tolerate so it was dropped. The reasons were based on blood biomarkers I’m guessing, nearly identical live donor match (my son), overall health. The side effects were the same as described here by many when taken for longevity. No matter what’s the purpose of taking it (longevity or something else), the sides are the same and point to the overly suppressed immune system (mouth ulcers, skin infections, flu like symptoms, activation of other dormant viruses, like herpes, fatigue, high lipids and glucose, etc.). Rapa accumulates quickly @1mg/day without washouts. I would say that sides appear after 2 weeks. I’m guessing that 0.5 mg if taken without breaks would work better. We need more research!
It was skin rash like contact dermatitis or eczema that looks like dry scratch-like marks (on shoulders or back), mouth ulcers, skin inflammation (acne-like on scalp), dry lesions after delayed wound healing that would leave a visible red mark for months. Those sides are usually resolved on Rapa breaks.My trough was 3.2-3.5 on 1 mg/day. My nephrologist didn’t want it to go lower than 3.
Hi Steve…rapamycin was misclassified as an immunosuppressant. It is actually an immunomodulator. When taken episodically, it enhances immune function. Ross
Hi out of interest would LDN work in a similar way but maybe less side effects? ‘LDN modulates the immune system. It doesn’t necessarily boost it, but it doesn’t necessarily suppress it to the point where we see issues of recurring infections.’
My current dose regime is 25mg once fortnightly. I combine it with a short fast to maximise autophagy. Looks like I might need to reconsider that approach!