For some reason all my posts were flagged by the community as spam?
If you search for treatment: Rapamycin and filter by completed studies there are 407 studies with results posted and 580 studies without result. I would post link but it won’t let me now.
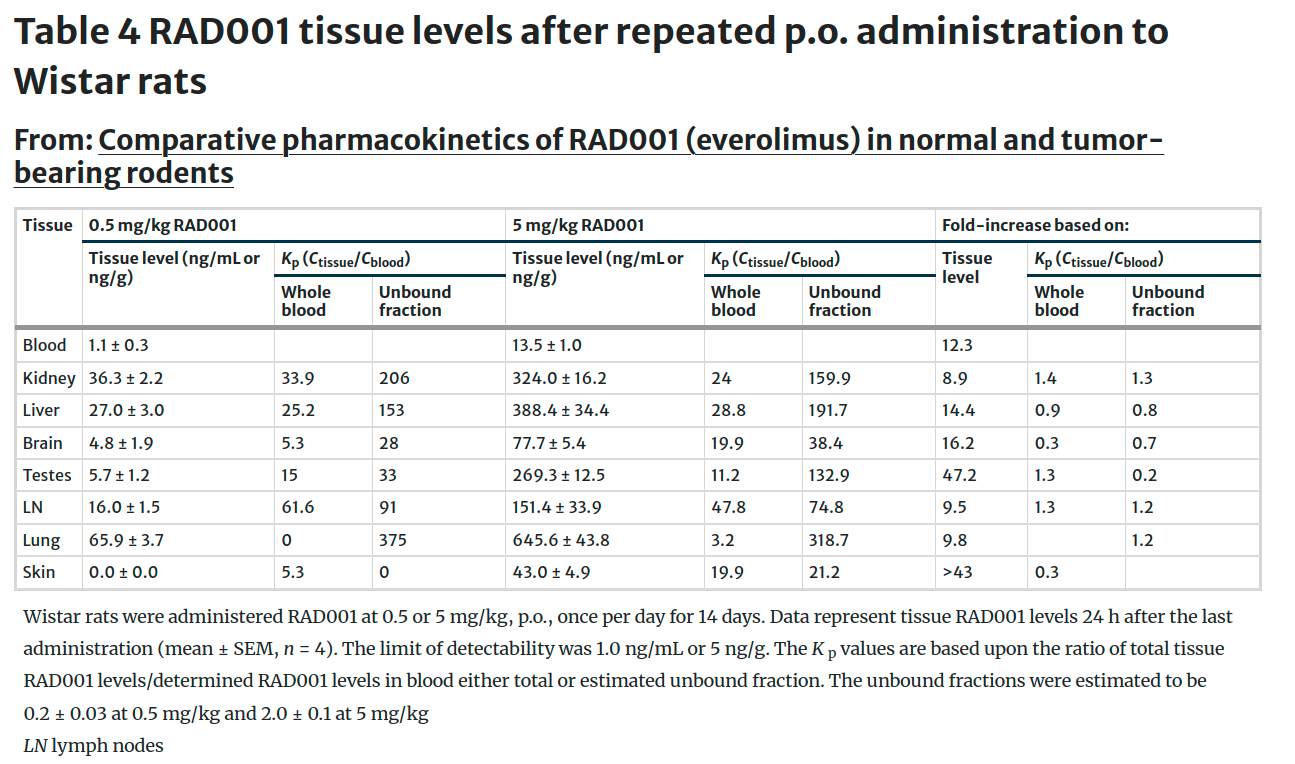
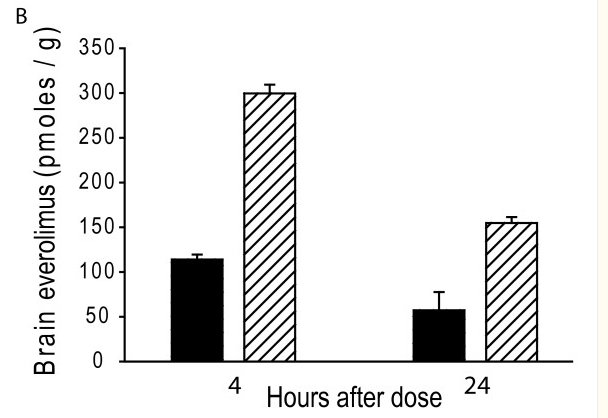
Here is another in mice (seems like high dose – 10 or 30 umol/kg aka 9 or 27 mg/kg but check my math). Also note that 100 pmoles/g is ~ 91 ng/g but again check my math.
Everolimus penetrates the blood-brain barrier in R6/2 HD transgenic mice . Plasma (A ) and brain (B ) everolimus concentrations were measured 4 and 24 hours after the last dose following two weeks of treatment (black-bar = 10 μmol/kg, cross-hatched bar = 30 μmol/kg).
The primary pathogenic mechanisms underlying neurodegenerative diseases such as Alzheimer’s disease (AD) involve neuroinflammation, oxidative stress and abnormal protein aggregation, while the main challenges facing effective treatment are limited drug targeting capabilities and the blood-brain barrier (BBB) that impedes drug delivery to damaged brain regions. To address these challenges, a nanosystem based on complexes of bioactive per se phosphorus dendrimers (AK-76) with hydroxyl surface groups and protein fibronectin (FN) with both targeting and therapeutic functions that were physically loaded with rapamycin was developed. The resulting R@A/F (R for rapamycin, A for dendrimer, and F for FN) nanocomplexes (NCs) with a size of 187.3 nm demonstrate good stability, cytocompatibility and targeting performance. We show that the R@A/F NCs can cooperatively modulate microglia by lowering reactive oxygen species level, restoring mitochondrial membrane potential, enhancing autophagy, promoting microglia M2 polarization, and suppressing inflammatory cytokine secretion in vitro. With the assistance of dendrimer terminal hydroxyl groups, the R@A/F NCs can cross the BBB and improve cognitive and memory impairments in an AD mouse model by reducing brain inflammation, stimulating autophagy and facilitating Aβ protein degradation. Our study offers a versatile and highly adaptable nanoplatform for advancing the combined treatment of neuroinflammatory diseases, thus representing a significant step forward in addressing the challenges of AD therapy.
I want to use rapamycin mainly for my brain so this is something I have wondered recently, is higher Area under curve or higher peak level more important for passing blood brain barrier?
It seems that if low levels of more frequent dosing of rapamycin passes BBB it may be better as it seems most neurodegenerative diseases may benefit from more constant mTOR inhibition than periodic dosing
This would be hard to measure. My approach and I probably take a higher dose than others, but very infrequently, is to be careful about increasing the dose. My last dose did not have any unusual side effects. Obviously I expect sleep disruption and high glucose etc and will probably be phoned by the lab when they find my WBC to be below 2G.
Also if I am getting sleep disruption I assume rapamycin is getting into the brain.
The only thing I ever heard was Blagosklonny’s position that a higher peak was better for passing the BBB. I assume that was a mechanistic assumption. I have followed a 2 week cycle with a “double dose” (~12-15mg) in part because of this position. I have no idea if it is right. I do not get sleep disruption as others report. I sleep better after a rapa dose.
Rapamycin doesn’t significantly cross the BBB. Why would higher doses help? (For sure, if 1% goes through the BBB and you take a mega dose, you’ll get some in the brain, but that will still be 1%.)
Kaeberlein… Attia all say the same. Hard to get anything across the BBB. And… personally… Blogsklonny might have been wrong about higher doses to achieve this.
Kaeberlein says that lowering inflammation at brain might be enough with the peripheral area of the brain getting benefits.
Even though it is for a single person (child) and not a big group, it seems here rapamycin must have passed the BBB sufficiently to induce such a big change especially given the patient was given about 1mg daily continuous (low dose daily).
The only thing I can think of is ASD patients have been shown to have weaker BBB at times which might have helped rapamycin get in, though it might not be the case here, as if the symptoms improved then the BBB should have also gotten stronger so it wouldnt have been a continuous improvement as seen in the study
Rapamycin need not cross the BBB for it to have an immediate and profound impact on the brain. Note the case of klotho. In the Peter Attia podcast on klotho, his guest, the scientist who conducted klotho studies, discussed the impact of klotho on the brain. Klotho does not cross the BBB. Yet in her studies in mice there is a profound effect of klotho on the brain function within four hours of administration, measurable by rigorous functional tests. The effects are apparently mediated by klotho altering blood factors, platelet activation in particular, which then cross the BBB and affect the brain.
In other words, you don’t need to have a drug/molecule cross the BBB to rapidly and strongly impact the brain, it can do so by modifying other factors which subsequently do cross the BBB and impact the brain. It is possible that rapamycin might work in a similar way, not by directly crossing the BBB, it can modify some other factors and thus affect the brain. Obviously I’m speculating, but the point is that crossing the BBB is not the deciding factor in evaluating the impact of any given molecule on the brain.
One interesting thing I learned about ketoconazole is that it inhibits P-glycoprotein (P-gp), a key efflux transporter at the BBB. Since sirolimus is a substrate of P-gp, ketoconazole is thought to increase sirolimus penetration into the brain by reducing its efflux. So in addition to ketoconazole’s effects on CYP3A4, it may also aid in raising sirolimus levels in the brain. I’m currently experimenting with a once every 21-day dose of 6mg sirolimus with 200mg ketoconazole (taken two hours prior). I plan to share my results so far in a separate post, but compared to weekly dosing with GFJ+EVOO, the difference is quite remarkable.
This successful trial of an immunosuppressant drug in PD shows that compounds that do NOT cross the BBB can still have a beneficial impact: Parkinson's disease - #730 by adssx
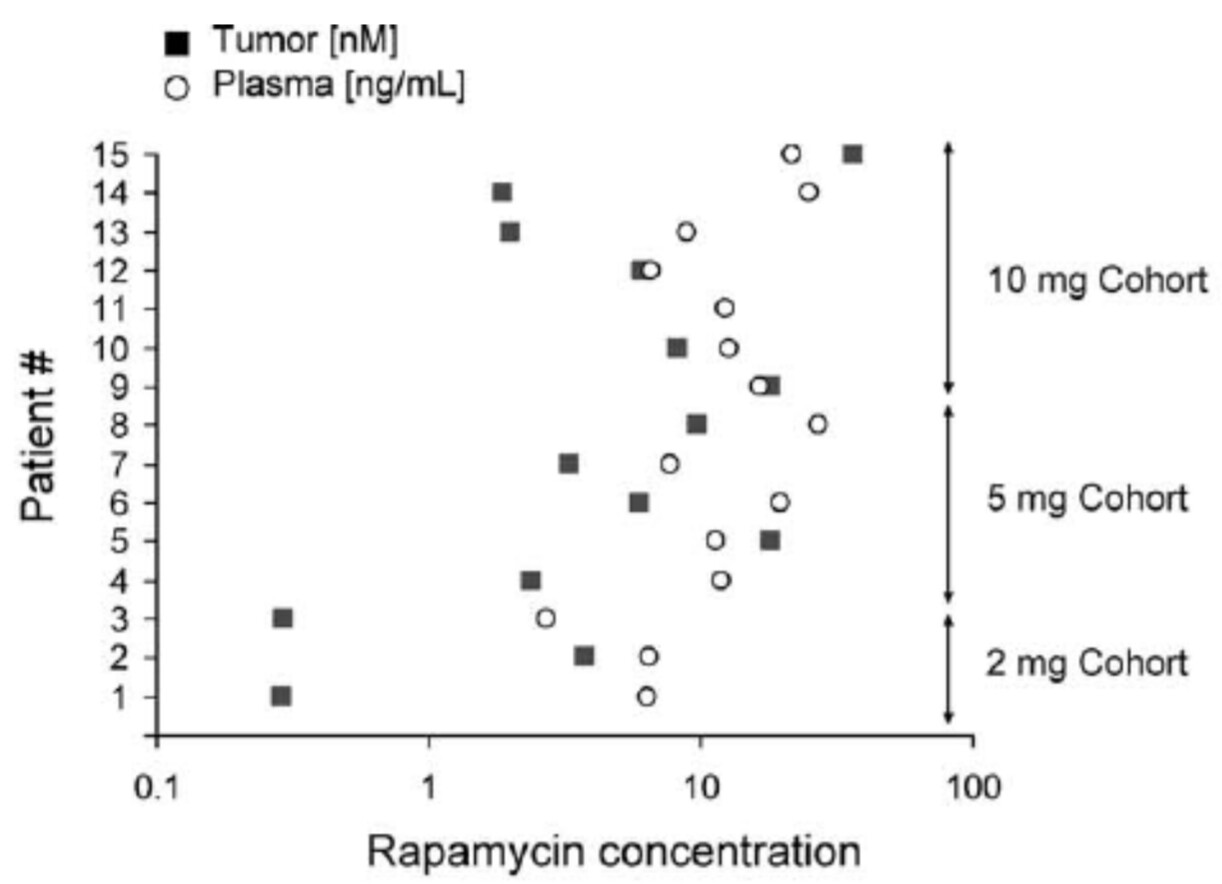
Looks like there is a huge individual variability but it clearly crossed the BBB.
The rapamycin doses are huge though: 2mg to 10mg per day for 7.5 days
For several patient the tumor concentration was 10+ times less than the plasma concentration but it’s better than nothing. Other patients had a higher concentration in the tumor than in the serum though.
Because rapamycin is a macrolide natural product whose
size could prevent distribution across the blood–brain
barrier, we measured rapamycin concentrations by mass
spectrometry in an aliquot of tumor tissue obtained at S2.
Rapamycin was detected in 14 of 14 tumors (insufficient
tissue was available from patient 11) at concentrations
ranging from 0.3–36.3 nM.