I think the point is you’d need to monitor … and do something consistently if you do this with grapefruit juice, pomegranate or other similar agents that inhibitor hepatic enzymes (ketoconazole - an antifungal agent also).
The issue is doing this with no monitoring seems risky, as suddenly getting 300-500% increase in Area under the curve from the same dose might be great in some settings - but you’d need to measure and carefully understand what you are doing, and do it the same way every time.
As much as rapamycin seems to have a great safety profile with cyclic dosing and moderate time of mTORC1 being active and same with mTORC2 - I’d think one would have to consider the risk of long term inhibition of both with adding grapefruit juice - and I think that is when the risk:benefit ratio of this whole thing starts to get me a little worried.
For some on this forum who are incredibly brilliant and can sort through all this and monitor, I suspect it could be safely done - I’d just not see it as something I’d recommend without careful mapping of the individual’s pharmokinetics with the exact preparation they are taking with exactly the same brand and quantity and frequency of the grapefruit … it could be done - but then the main benefit would be a lower dose to achieve the desired outcome, but if the half life is prolonged, one still has to battle with having inhibition that is longer than desired.
That would be my take on this. A great hack for cancer patients, but not so sure it is a win with longevity uses.
Thank you for the answere. I just did not know that pomegranate was a CYP3A4 inhibitor. It was a very important information for me (this since I use pomegranate). I have to find out more about that, and how strong inhibitor it is.
It might be of interest to the group here that sildenafil is metabolised by CYP3A4.
“Sildenafil is metabolized mainly by CYP3A4 (79%) and, to a lesser extent, by CYP2C9 (19%) [30]. Since pomegranate constituents impair CYP2C9, this may be the main reason for increasing sildenafil bioavailability and therefore prolonging the erection period. In addition, the delay in absorption may be related to pomegranate interaction with CYP3A4.”
I have learned some very useful information today. I take pomegranate and also sildenafil. Thanks a lot.
Maybe this should be in a thread about bioavailability and the metabolism of rapamycin. I make one last post that might be of value for some here. It might be good to know thst. Grapeseed extract and Green tea extract also have effect on CYP3A4.
“The cancer chemoprevention potential and anticancer efficacy of many herbal products such as grape seed (GS) and green tea (GT) extracts had led to an increase in their concomitant use with anticancer agents. GS and GT extracts were demonstrated to be potent inhibitors of CYP3A4”
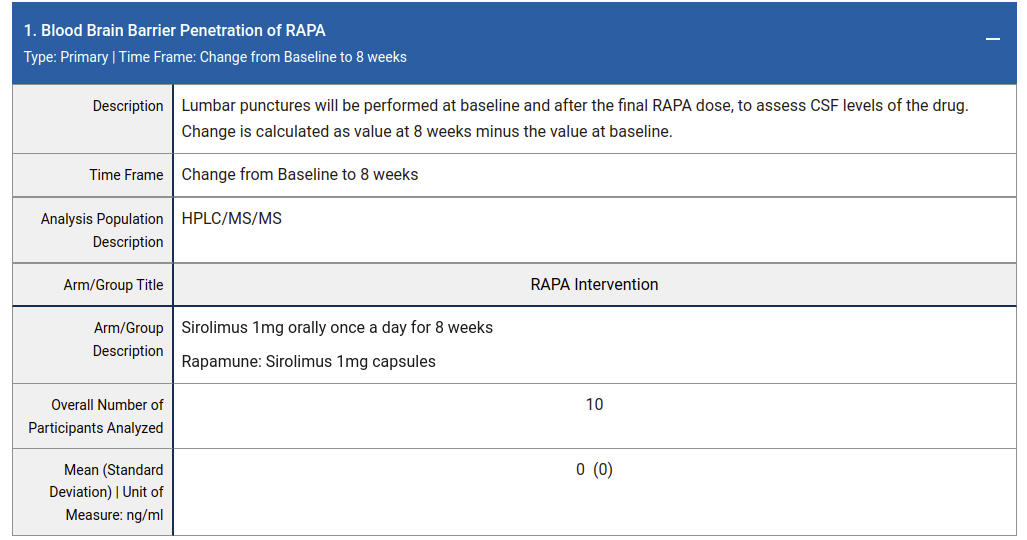
Here is a clinical trial of 1mg/day Rapamune for 8 weeks in patients with MCI or early AD where they measured rapamycin contentration in CSF. They didn’t find any (0 ± 0 ng/mL):
A pertinent question is does Rapamycin cross the BBB at dosages used in mouse studies. If not, the brain benefits may not rely on BBB penetration but could be mediated systemically (e.g. reduced inflamation, directly at the endothelial cells of BBB, etc). For example, 14 ppm rapamycin (~2.24 mg/kg/day) has substantial benefits in APOE4 transgenic mice on the BBB integrity. This is ~1/2 the dose of the study that @RapAdmin posted above where Rapamycin was undetectable in the brain.
I wonder if the brain tumor rapamycin data might be misleading (does a brain tumor have a similar BBB as does healthy brain tissue?).
Where do you see the results from this study? Please provide a link.
1mg/day for 8 days seems like an extremely low dose (or at least a short period and very moderate dose). Perhaps its the “bolus” type dosing (10mg to 20mg at once) that gets it past the blood brain barrier.
All the rapamycin researchers I’ve spoken to say they see penetration of the BBB even in pretty low doses in model organisms (mice, marmosets, etc.)… so this result you suggest is surprising.
It was 1mg/day for 8 weeks, not 8 days. The link is right under the table in my post above (here again).
Maybe a bolus dose does get into the brain but we don’t know without data. Do you have any relevant publications which show BBB penetration in model organisms at low doses?
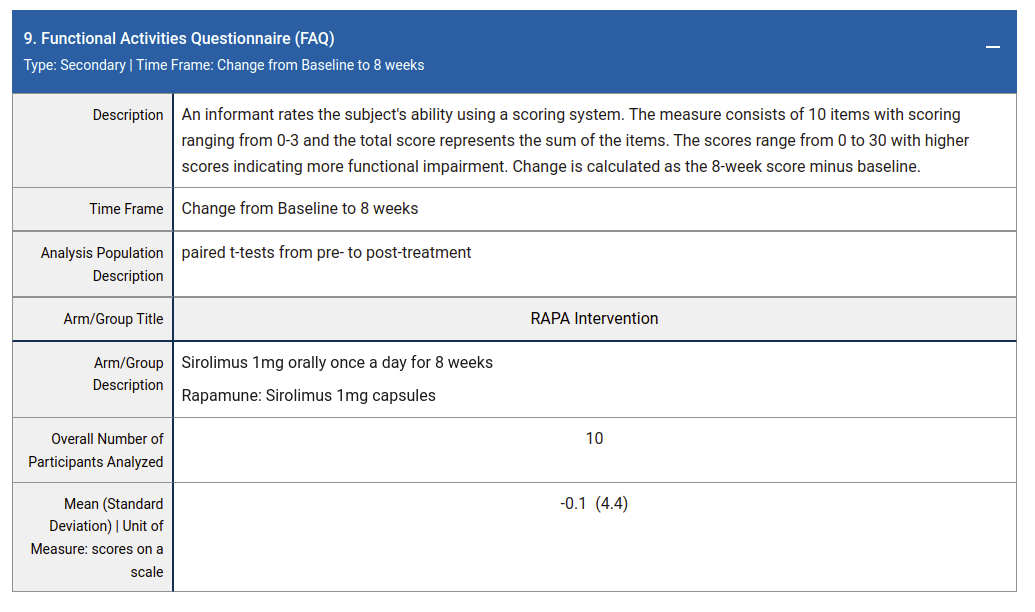
There is no publication listed on the clinical trial record but the results are not default data (all other results related to cognition, adverse events etc are complete). The results themselves don’t look particularly compelling (perhaps why it isn’t published).
Sorry - yes, 8 weeks. But still, 1 mg/day is a pretty low dose.
I see and reviewed the link to the clinical trials.gov info - but while I may have missed it, those entries typically don’t publish the results of the studies, and I don’t see a link to any papers published based on the study. Did I miss that?
Yes - I find this really surprising. I’ve actually never seen results data published on the ClinicalTrial.gov website and didn’t (and still don’t really know) that they publish the actual results there. I thought all the results from these clinical studies was only published in follow-on papers (if at all).
I have no confidence that the results reported there are what @alexvpickering is interpreting them as. So - I’ve emailed Mitzi the PHD contact at the study to see if it is correct.
So either it’s a problem of patients with MSA, or, even in healthy people, no matter whether sirolimus crosses the BBB, it does not inhibit brain mTOR.
For some reason all my posts were flagged by the community as spam?
If you search for treatment: Rapamycin and filter by completed studies there are 407 studies with results posted and 580 studies without result. I would post link but it won’t let me now.
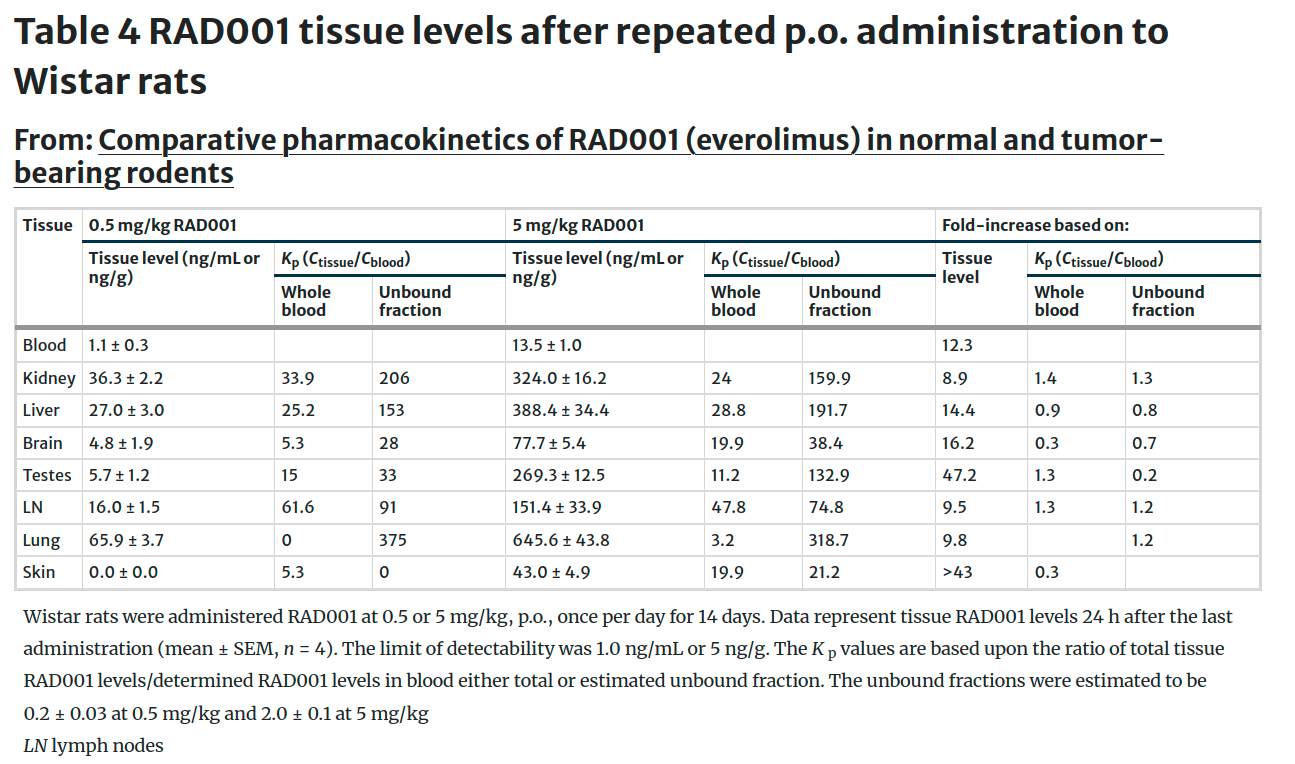
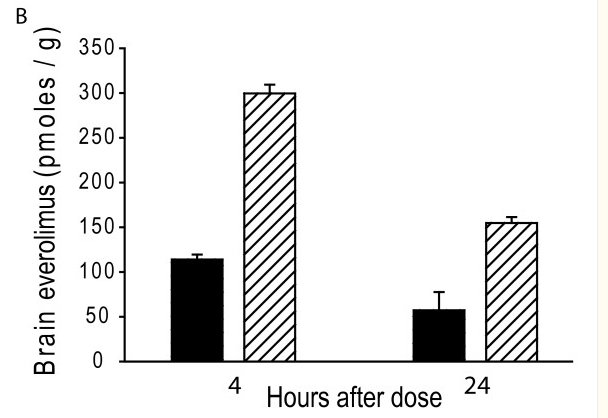
Here is another in mice (seems like high dose – 10 or 30 umol/kg aka 9 or 27 mg/kg but check my math). Also note that 100 pmoles/g is ~ 91 ng/g but again check my math.
Everolimus penetrates the blood-brain barrier in R6/2 HD transgenic mice . Plasma (A ) and brain (B ) everolimus concentrations were measured 4 and 24 hours after the last dose following two weeks of treatment (black-bar = 10 μmol/kg, cross-hatched bar = 30 μmol/kg).