To come back to this. I didn’t do a blinded test on myself, but, I took a higher rapamycin dose (2mg) and it had no discernible effect on me, maybe an effect on my sleep.
I also did a 3-day fast a week prior to the 2mg rapamycin dosage and again, no hallucinations/anxiety.
My small theory on what contributed to the anxiety/hallucinations that time:
Most likely: 1. It was my first 3-day fast and my first time entering ketosis. I think my body just struggled a little and I became hypoglycemic.
May have played a role: 2. My electrolytes intake wasn’t on point. (Hand numbness when my arm was higher than my heart) in proceeding fasts I found out it was my potassium : sodium ratio, so I adjusted and that fixed it.
As part of this thread, this new podcast is interesting with respect to rapamycin use. If increased permeability of the blood brain barrier is a key early indicator of dementia, I wonder how that maps to rapamycin’s penetration into the brain (and benefits thereof).
Are these results generalizable to non-MSA patients? Is rapamycin less potent in the brain? Does rapamycin inhibit brain mTOR?
The trial tested rapamycin daily instead of once weekly or once every two weeks: could a higher interval let rapa cross the BBB and work on brain mTOR?
Are there other drugs out there that inhibit brain mTOR? Maybe SGLT2 inhibitors? SGLT2i bind to mTOR in the same structural domain used by rapamycin (source). They cross the BBB. Among SGLT2i, empagliflozin has the highest brain-to-serum ratio, 0.5 (see Neuroprotective Effect of SGLT2 Inhibitors) vs 0.0057 for rapamycin (per source): 87x more!
Thanks. Are there studies quantifying this? It would be interesting to measure brain mTOR inhibition with rapa 20-mg once every 2w vs, for instance, empagliflozin 10mg daily. SGLT2i cross the BBB so much more easily that it may compensate for their lower mTOR inhibition properties.
Besides SGLT2i, it seems that GLP1 agonists, and especially exenatide, can significantly inhibit brain mTOR: “Exenatide treatment was demonstrated to increase tyrosine phosphorylation of IRS-1, an effect that was associated with changes in the downstream effectors, Akt, and mTOR. Furthermore, levels of mTOR were demonstrated to associate with the level of clinical benefit. Thus, augmentation of insulin signalling may underlie the neuroprotective effects of exenatide. Engagement of AKT and mTOR pathways may prevent α-synuclein aggregation, protect dopaminergic neurons, reduce inflammation, and enhance cell survival.” (Antidiabetic agents as a novel treatment for Alzheimer’s and Parkinson’s disease 2023)
Not sure about that. They seemed to be speaking from direct experience with mice experiments. They mentioned the rapa molecule almost needed to be pushed through the BBB via back to back high dosages for a while — rough human equivalent to three consecutive days of 10-20g. Basically it had to be in the blood continuously for a considerable while as both the large molecular size and the lipophilicity made it hard.
A couple of things here - we really need to consider whether higher doses are necessary to get good levels in the brain. I think the consensus from my reading on this (and I’m not going to cite all the references) is that it is likely that a higher dose is more likely to generate significant levels in the brain.
So if we are willing to accept that premise, the issue becomes safe dosing and also with the theory that we might want a ratio of 1:2 on high levels of mTORC1 inhibition:little mTORC1 inhibition.
This is where I think we need to look at the formulation someone is on, and actually need to sort out their individual half life of rapamycin and check this as the dose goes up. Looking at total level of sirolimus ~20 hours post dose, then checking again in 36 hours can give us a solid basis to understand half life, and understand when mTORC1 inhibition is likely to be minimal. That can then help establish dosing interval when we start looking at these bigger doses.
Single doses of Rapamycin likely have a T1/2 of 36 hrs or so, daily dosing is quoted at 64 hrs. Does a really large single dose act more like 36 hrs or 64 hrs? Does this differ between individuals (e.g. elderly and liver dysfunction can prolong to over 100 hrs) or the formulation?
For my patients on this, especially for high dose cyclic for neurological disease, there must be testing to understand the pharmacokinetics in a given person to then consider dose and interval.
Grapefruit juice brings in a totally crazy risk (as does pomegranate) of knowing it will unpredictably affect levels and half-life, but if anything will prolong the half-life, probably with repetitive dosing of the grapefruit - but throws a monkey wrench of unpredictability into the equation. I’d not mix the two as this is already on the cutting edge of longevity medicine - and there is clearly an increased risk under mTORC1 inhibition of having bacterial infection that your body is inadequately going to respond to.
One doesn’t want to accidentally off themselves while trying to live longer!
I think the point is you’d need to monitor … and do something consistently if you do this with grapefruit juice, pomegranate or other similar agents that inhibitor hepatic enzymes (ketoconazole - an antifungal agent also).
The issue is doing this with no monitoring seems risky, as suddenly getting 300-500% increase in Area under the curve from the same dose might be great in some settings - but you’d need to measure and carefully understand what you are doing, and do it the same way every time.
As much as rapamycin seems to have a great safety profile with cyclic dosing and moderate time of mTORC1 being active and same with mTORC2 - I’d think one would have to consider the risk of long term inhibition of both with adding grapefruit juice - and I think that is when the risk:benefit ratio of this whole thing starts to get me a little worried.
For some on this forum who are incredibly brilliant and can sort through all this and monitor, I suspect it could be safely done - I’d just not see it as something I’d recommend without careful mapping of the individual’s pharmokinetics with the exact preparation they are taking with exactly the same brand and quantity and frequency of the grapefruit … it could be done - but then the main benefit would be a lower dose to achieve the desired outcome, but if the half life is prolonged, one still has to battle with having inhibition that is longer than desired.
That would be my take on this. A great hack for cancer patients, but not so sure it is a win with longevity uses.
Thank you for the answere. I just did not know that pomegranate was a CYP3A4 inhibitor. It was a very important information for me (this since I use pomegranate). I have to find out more about that, and how strong inhibitor it is.
It might be of interest to the group here that sildenafil is metabolised by CYP3A4.
“Sildenafil is metabolized mainly by CYP3A4 (79%) and, to a lesser extent, by CYP2C9 (19%) [30]. Since pomegranate constituents impair CYP2C9, this may be the main reason for increasing sildenafil bioavailability and therefore prolonging the erection period. In addition, the delay in absorption may be related to pomegranate interaction with CYP3A4.”
I have learned some very useful information today. I take pomegranate and also sildenafil. Thanks a lot.
Maybe this should be in a thread about bioavailability and the metabolism of rapamycin. I make one last post that might be of value for some here. It might be good to know thst. Grapeseed extract and Green tea extract also have effect on CYP3A4.
“The cancer chemoprevention potential and anticancer efficacy of many herbal products such as grape seed (GS) and green tea (GT) extracts had led to an increase in their concomitant use with anticancer agents. GS and GT extracts were demonstrated to be potent inhibitors of CYP3A4”
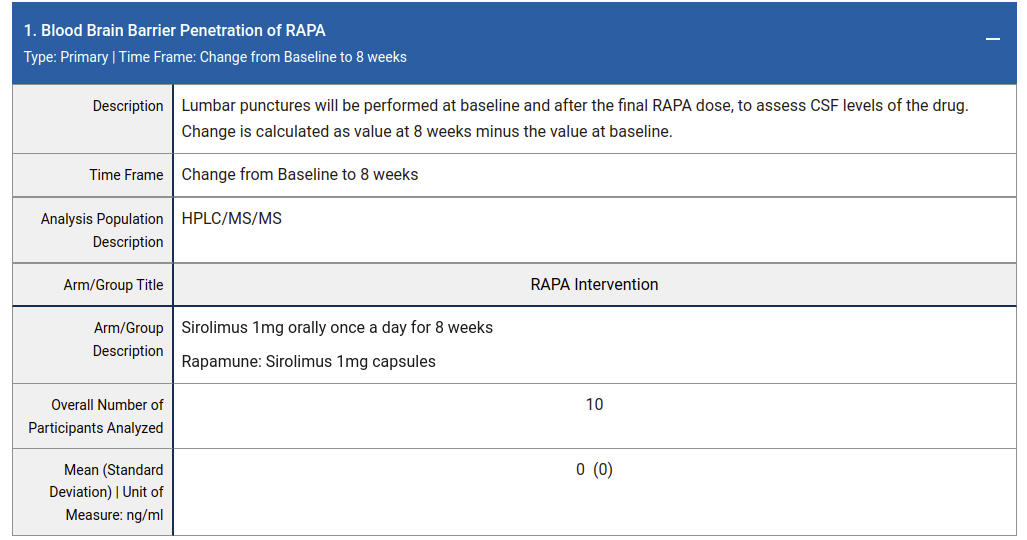
Here is a clinical trial of 1mg/day Rapamune for 8 weeks in patients with MCI or early AD where they measured rapamycin contentration in CSF. They didn’t find any (0 ± 0 ng/mL):
A pertinent question is does Rapamycin cross the BBB at dosages used in mouse studies. If not, the brain benefits may not rely on BBB penetration but could be mediated systemically (e.g. reduced inflamation, directly at the endothelial cells of BBB, etc). For example, 14 ppm rapamycin (~2.24 mg/kg/day) has substantial benefits in APOE4 transgenic mice on the BBB integrity. This is ~1/2 the dose of the study that @RapAdmin posted above where Rapamycin was undetectable in the brain.
I wonder if the brain tumor rapamycin data might be misleading (does a brain tumor have a similar BBB as does healthy brain tissue?).
Where do you see the results from this study? Please provide a link.
1mg/day for 8 days seems like an extremely low dose (or at least a short period and very moderate dose). Perhaps its the “bolus” type dosing (10mg to 20mg at once) that gets it past the blood brain barrier.
All the rapamycin researchers I’ve spoken to say they see penetration of the BBB even in pretty low doses in model organisms (mice, marmosets, etc.)… so this result you suggest is surprising.
It was 1mg/day for 8 weeks, not 8 days. The link is right under the table in my post above (here again).
Maybe a bolus dose does get into the brain but we don’t know without data. Do you have any relevant publications which show BBB penetration in model organisms at low doses?
There is no publication listed on the clinical trial record but the results are not default data (all other results related to cognition, adverse events etc are complete). The results themselves don’t look particularly compelling (perhaps why it isn’t published).