No noticeable side effects at all, but my LDL is high - so I need to watch that and may restart statins.
Re LDL, as part of general lipid dysregulation?
And this was only after Rapamycin dosing? You controlled for other reasons?
Can you share your TG/HDL and remnant cholesterol and units? The latter is TC-LDL-HDL.
These are two very good proxies for CVD risk stratification.
My Total and LDL numbers have gone up about 50 points since starting rapamycin.
Here are the numbers (in a fasted state):
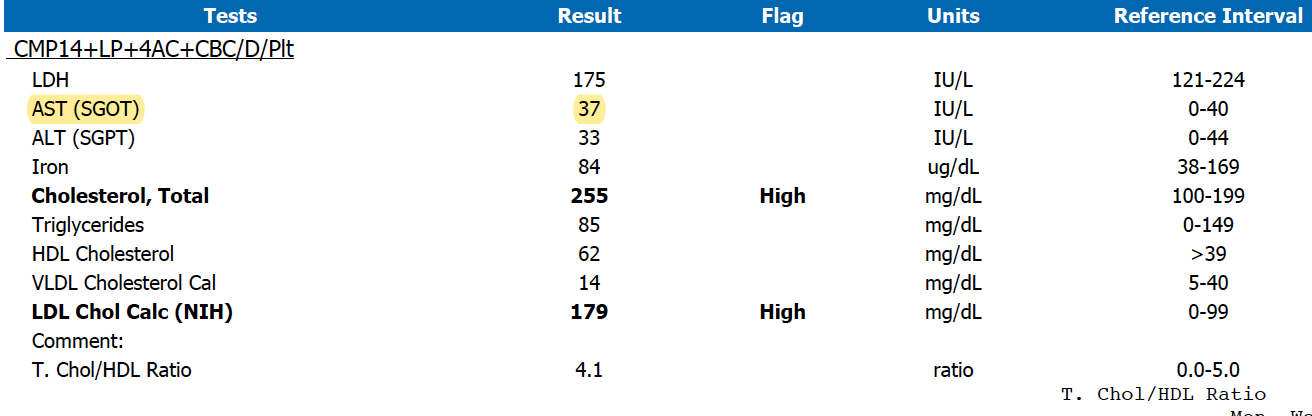
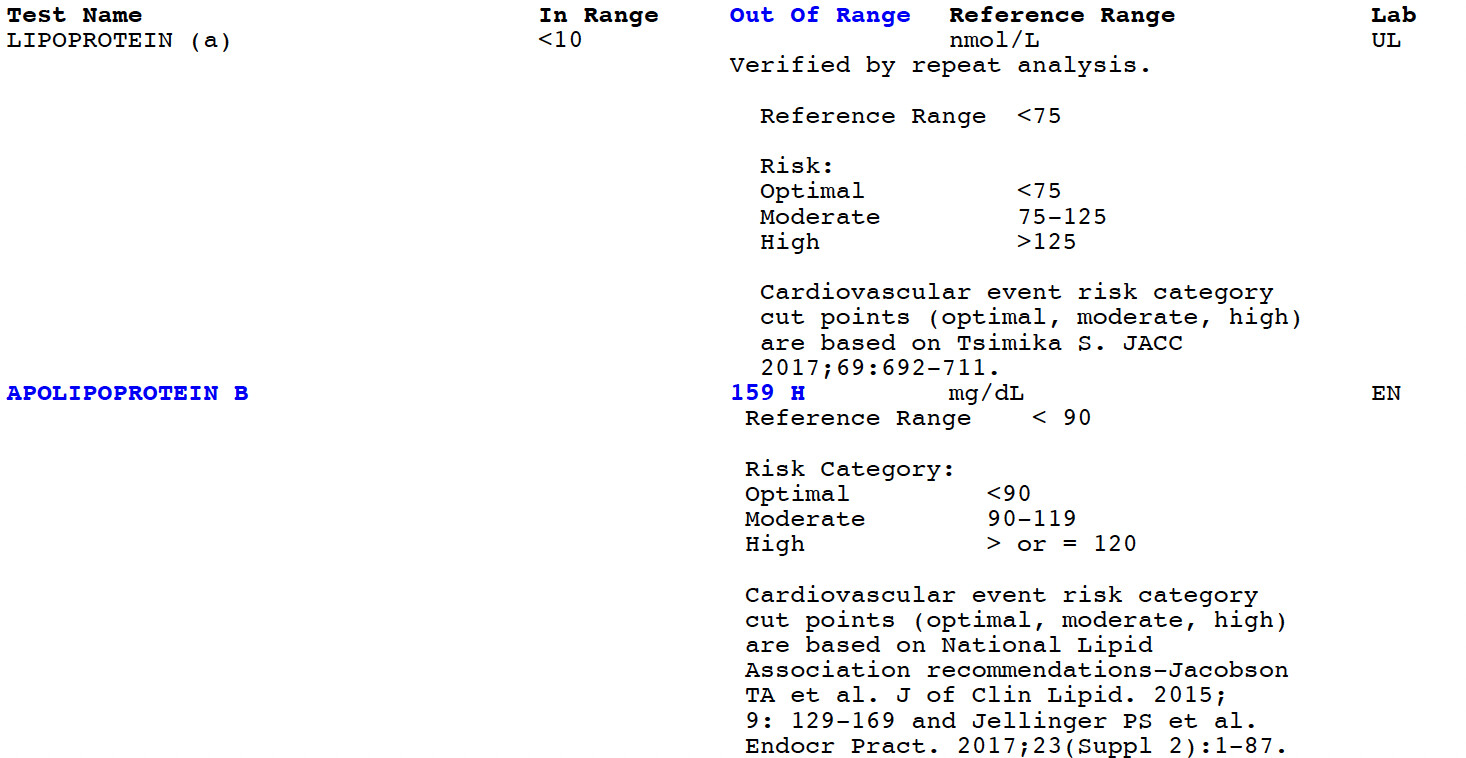
Here are my Lipo A, and APO B numbers:
1 Like
My research on remnant cholesterol suggests that my level of approx. 14mg/dL puts me in the low risk category according to the studies I’ve seen (see below) - but my LDL numbers put me in a higher risk, as does my T.Chol/HDL Ratio.
RESULTS:
Median calculated remnant cholesterol was 0.40 mmol/L [interquartile range (IQR), 0.30 – 0.55 mmol/L] [15 mg/dL (12–21 mg/dL)] for underweight,
0.50 mmol/L (IQR, 0.37–0.71 mmol/L) [19 mg/dL (14 –27 mg/dL)] for normal weight
Stepwise higher remnant cholesterol was associated with stepwise higher myocardial infarction risk in a similar pattern for normal weight, overweight, and obese individuals. When compared with individuals with remnant cholesterol 0.5 mmol/L (19 mg/dL), individuals with remnant cholesterol 1.5 mmol/L (58 mg/dL) had hazard ratios for myocardial infarction of 2.0 (95% CI, 1.3–3.2) for normal weight
From this paper: Remnant Cholesterol and Myocardial Infarction in Normal Weight, Overweight, and Obese Individuals from the Copenhagen General Population Study
Why do you not workout after Rapa dosing, I’m curious…
RapAdmin, your ApoB is the single most important number out of everything, since your Lp(a) is low. Peter Attia’s latest AMA from this week goes into ApoB, as do some of his previous podcasts. ApoB is a better measure of risk than the amount of cholesterol in your LDL. You’ve got to get that down. If you want to avoid potential risks of statins yet potentially bring it down significantly, you could try citrus bergamot and/or amla extract. Ezetimibe is also a great, cheap and safe generic med but likely won’t be enough by itself.
3 Likes
I am NOT a medical professional, just sharing some CVD knowledge.
Quick comment on liver enzymes…have you not seen them go down with Rapamycin?
Yes, your RC of 14 mg/dL puts you in the lowest risk bracket.
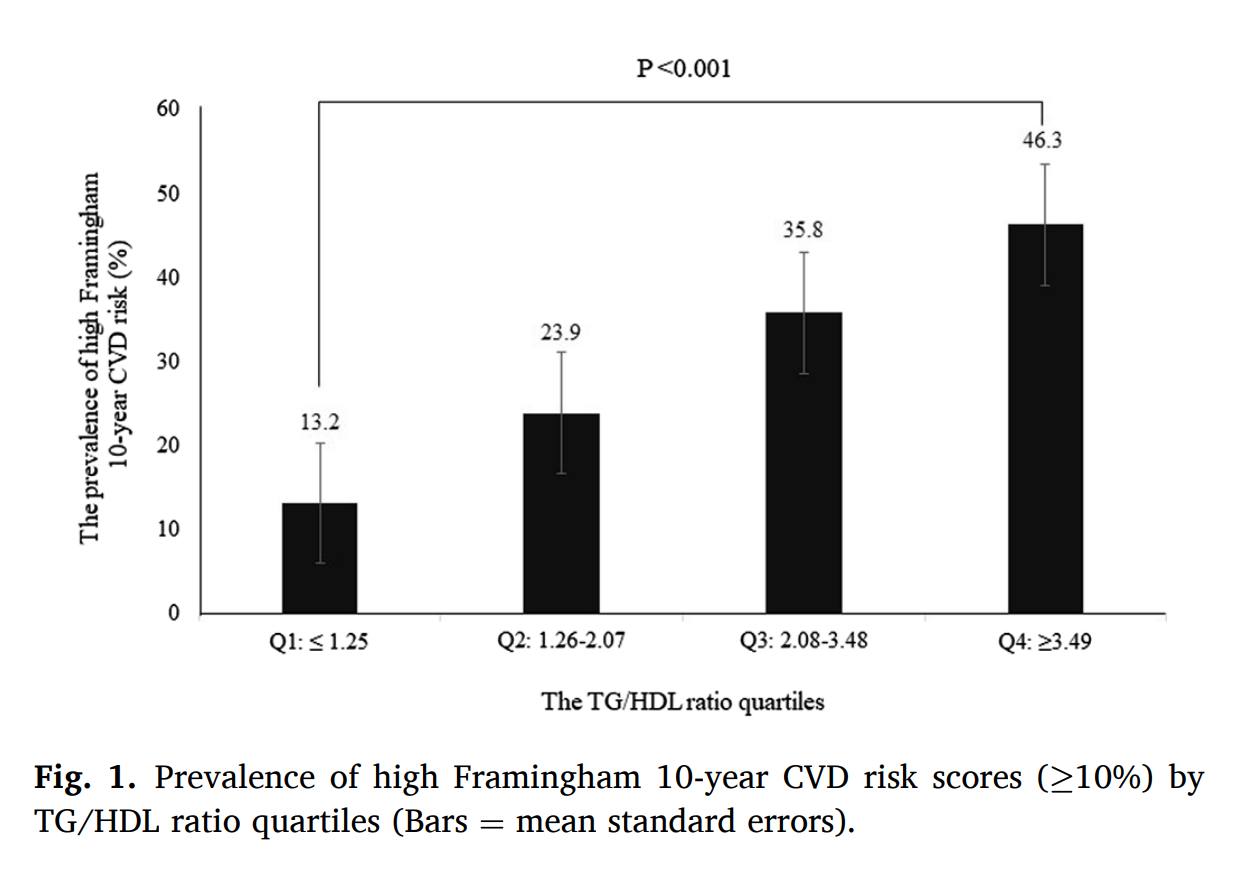
Your TG/HDL = 1.37. This is in a relatively lower risk quartile. TG/HDL correlates with small atherogenic LDL particle number.
https://sci-hub.se/https://doi.org/10.1016/j.cca.2021.05.029
https://sci-hub.se/http://dx.doi.org/10.1136/jim-2018-000869
Since you have an apoB result, some further insight.
Your high APOB, high LDL, and high non-HDL-C (TC-HDL-C) is a RISK factor…they are concordantly high.
Can I ask your age, BMI, hbA1c? Hypertension?
Have you ever had a CIMT or CCAC to assess actual cardiovascular atherogenicity?
Best to review all this with your family doctor/cardiologist.
Discordance Between Apolipoprotein B and LDL-Cholesterol in Young Adults Predicts Coronary Artery Calcification: The CARDIA Study
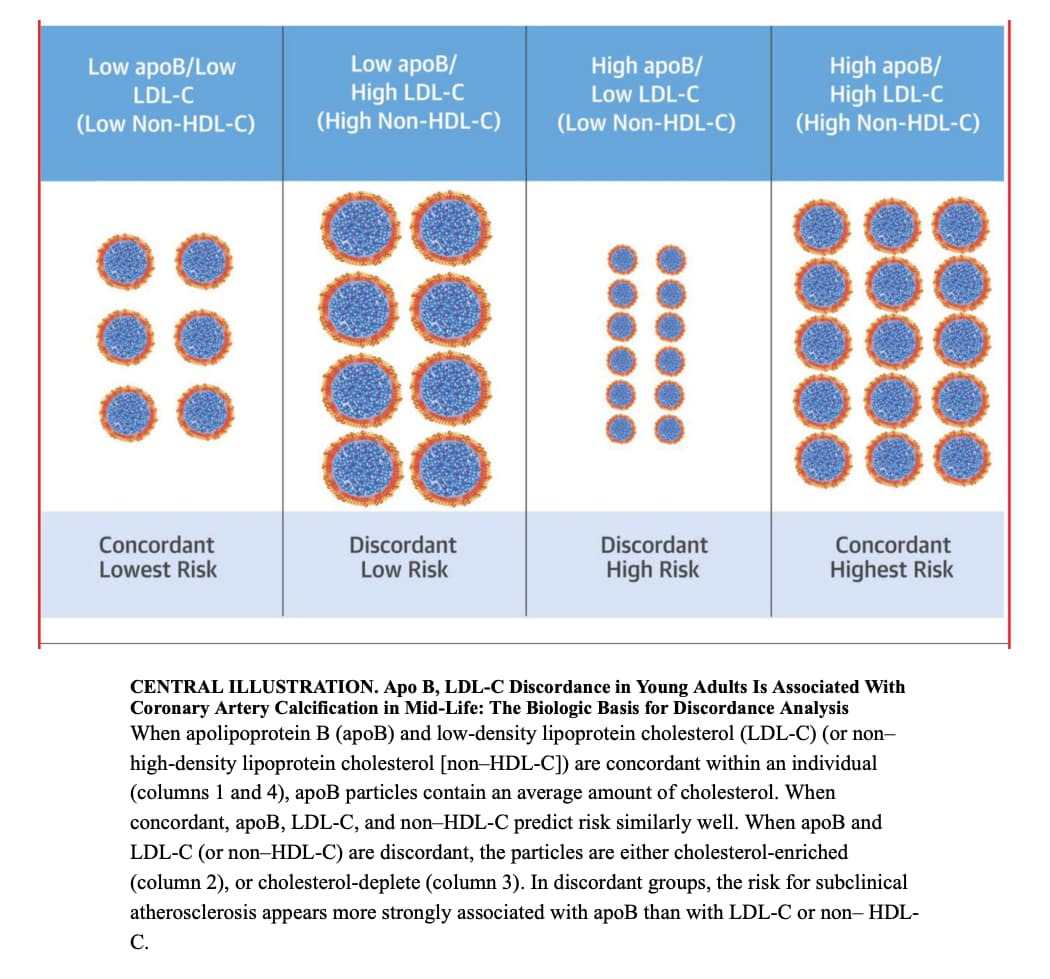
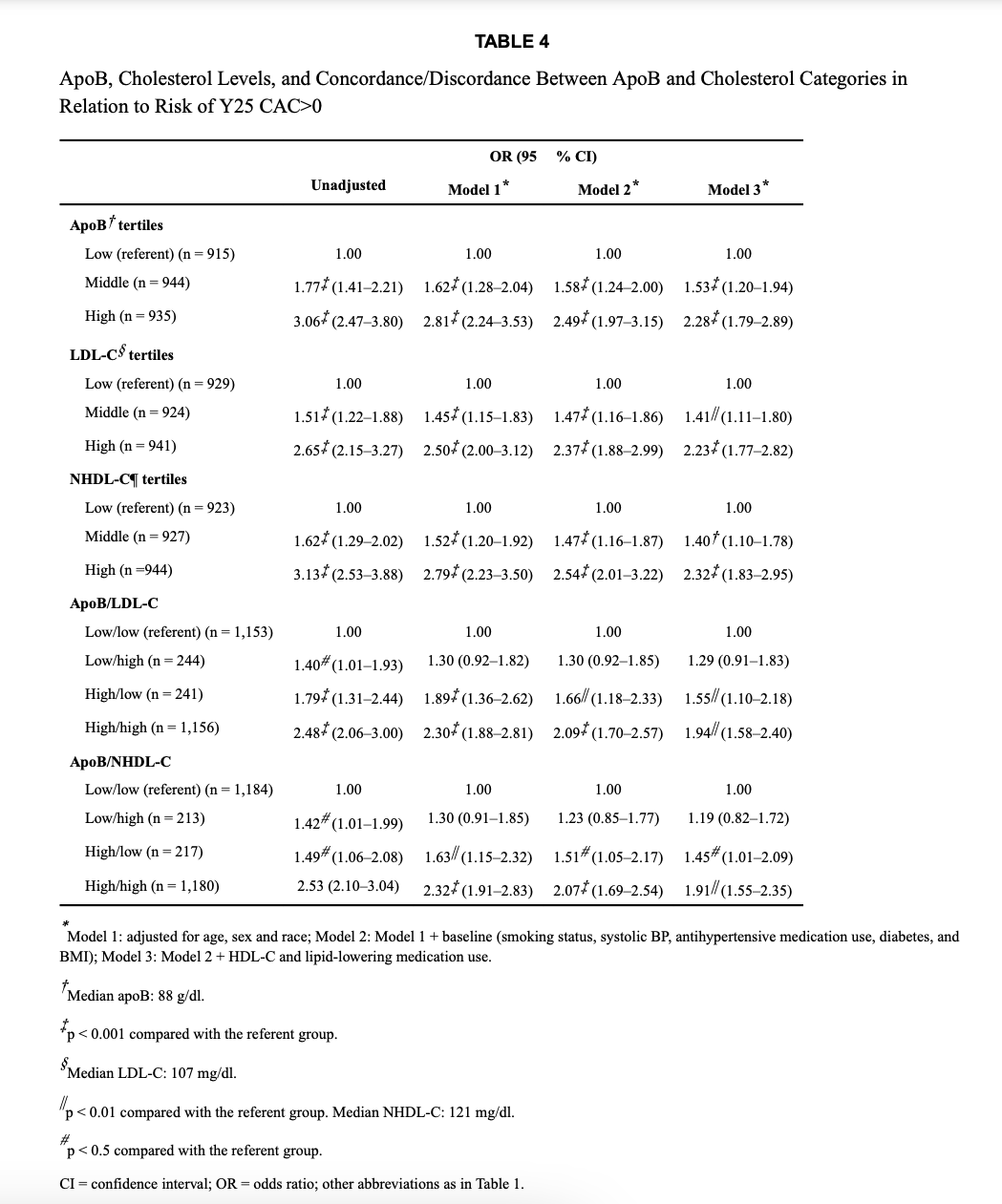
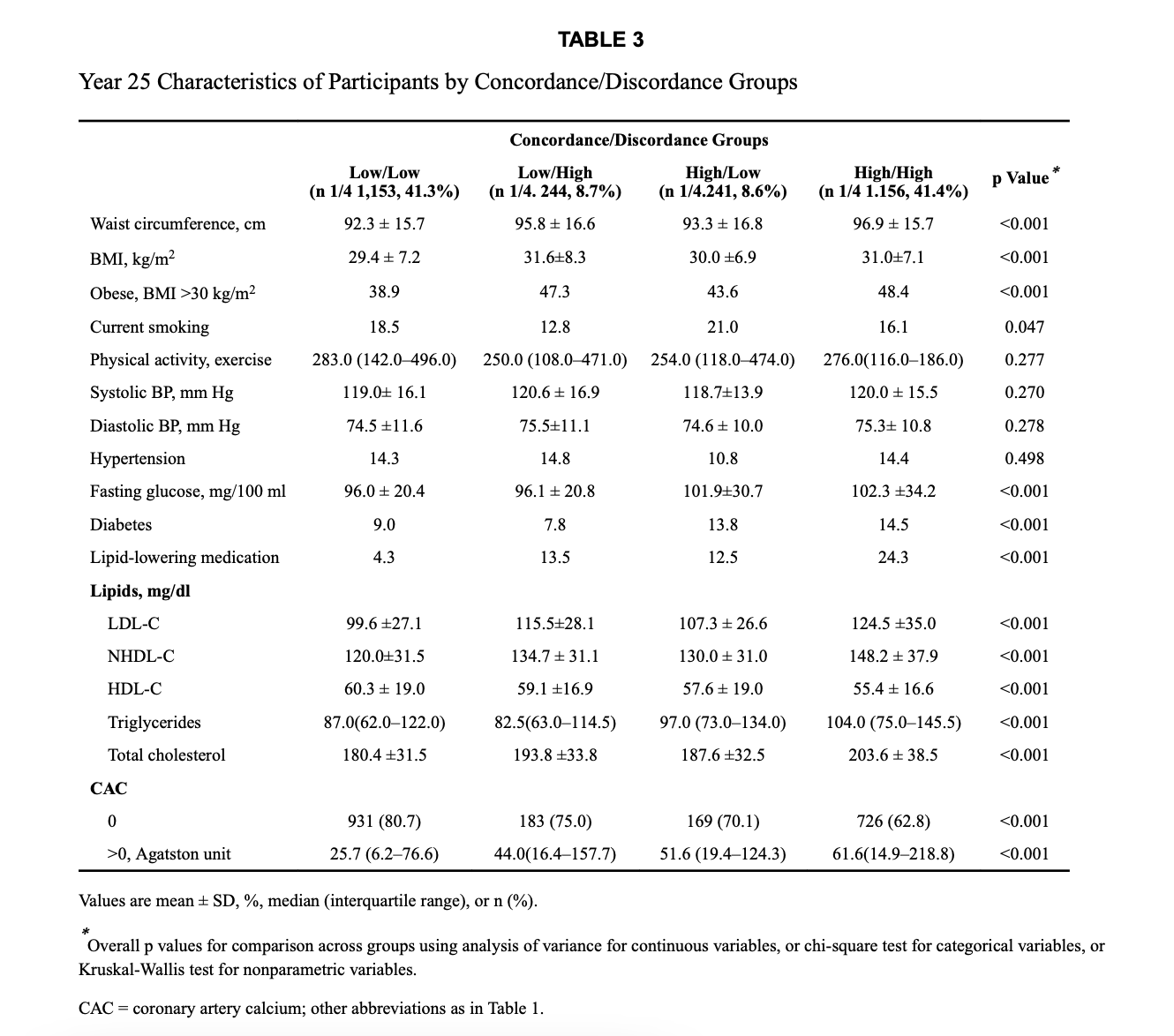
Here is another reference, indicating risk of high APOB/high LDL-C, and high non HDL-C.
3 Likes
Just noticed your article on sleeping. Excellent work, with all the cites. I am almost 76, and just like you have had trouble staying asleep at night. Here in Spain, I can get this without Rx, and only costs 3.17 euros for 30 100 mg tabs. Will let you and group know how it goes. I currently tak 20 mg. rapa twice a month, and have been on rapa sincel March 2017. We all know that quality sleep is very important.
1 Like
Here is a very good reason to take a low dose statin, to lower inflammation in the body which goes up as we age. Inflammation causes plaque buildup and can turn calcified plaque into hot plaque which can cause heart attacks and strokes. I personally take 5 mg. crestor daily and my C-reactive is less than .01. Save your kidneys, heart, and brain from plaque buildup with a low dose statin. Here is a lengthy video on the subject. Statins and CV Inflammation: The real impact on plaque (LIVE) - YouTube
2 Likes
Still another reason to take low dose statins:
“Twenty-five studies met eligibility criteria. Use of statins was significantly associated with a reduced risk of all-caused dementia.”
“Use of statins and the risk of dementia and mild cognitive impairment: A systematic review and meta-analysis”
https://www.nature.com/articles/s41598-018-24248-8
1 Like
It seems that it would be a really interesting study to see if rapamycin use shifts the sleep phenotype to a more youthful state…
I doubt anyone has done this before - but from my own experience I think this might be true.
2 Likes
You might be onto something.
Actually I have discovered my dreams since rapa (starting at about 1 year of use) have gone from few and un-memorable to very colorful… almost lucid… and I remember them long after I had them. In my youth that’s how my dreams were.
FYI.
6 Likes
Yeah that would be interesting to do, although the study itself would be hard and probably time consuming. I guess we would have to define what youthful state would be as well.
1 Like
I think it would be really interesting because it might be one way to measure Rapamycin’s “anti-aging” effect on the brain non-invasively and quite quickly (compared to most measures of aging… like disease incidence)…
I have to believe that the profile of normal, healthy sleep patterns has been pretty well characterized for people age 40 or 50 years, and probably also in the elderly, from past studies. All we need to do is do a pre and post study of a sample of people age 60 to 80, with and without rapamycin (say 6 mg/week) , similar in concept to the resTORBio trial for flu vaccination…
But yes - perhaps something more likely funded by the Impetus grants, than the NIA.
" In healthy adults, sleep typically begins with NREM sleep. The pattern of clear rhythmic alpha activity associated with wakefulness gives way to N1, the first stage of sleep, which is defined by a low-voltage, mixed-frequency pattern. The transition from wakefulness to N1 occurs seconds to minutes after the start of the slow eye movements seen when a person first begins to nod off. This first period of N1 typically lasts just one to seven minutes. The second stage, or N2, which is signaled by sleep spindles and/or K complexes in the EEG recording, comes next and generally lasts 10 to 25 minutes. As N2 sleep progresses, there is a gradual appearance of the high-voltage, slow-wave activity characteristic of N3, the third stage of NREM sleep. This stage, which generally lasts 20 to 40 minutes, is referred to as “slow-wave,” “delta,” or “deep” sleep. As NREM sleep progresses, the brain becomes less responsive to external stimuli, and it becomes increasingly difficult to awaken an individual from sleep."
https://healthysleep.med.harvard.edu/healthy/science/what/sleep-patterns-rem-nrem
1 Like
I take my rapamycin once a week … always before bed… 10mg with GFJ.
It is always a very restless night. Just is… lol.
Next night I sleep fine.
1 Like
I normally take the dose in the AM, not noticed any discernible impact. Once, travelling, I mistakenly took a dose before bed, I could NOT fall asleep.
3 Likes
Hahaha, exactly!
Not surprised at all. My sleep is broken… confused… time goes slowly… based on checking the clock.
It’s interesting to see the various results and effects people have on this new frontier journey we are taking.
I am 81 yrs old, and as you are well aware, the older you get the more trouble you have getting a good night’s sleep.
As I have posted earlier I have had some various and long “sleep stacks” that I was taking.
My experience with rapamycin is that for the first few months of taking rapamycin. (starting dose of 5mg. weekly) I felt no sleep effects one way or another while taking these lower doses in the morning.
I have been ramping (titrating) up the dose from 5mg weekly to a high of 20mg. with grapefruit juice bi-weekly. I had to back off because the 20 mg dose was giving me diarrhea. Then I switched to 10mg/weekly with grapefruit juice weekly with no unpleasant effects. Now I am have been taking 12mg. weekly for the last two doses with no unpleasant effects.
At about the time I started taking the 12mg. weekly dose I notice I was sleeping too soundly and waking up too slowly. What is too soundly for me? Too soundly for me means not moving enough to prevent getting pains from sleeping in the same position.
So, I decided to reduce my “sleep stack” to 3mg. of melatonin and 2 grams of tryptophan.
This the best sleep I have gotten for years. I really think the time, 5+ months, and higher doses of rapamycin may have done the trick.
6 Likes