Thanks, is there a manufacturer that you trust for Ezetimibe coming from india?
Ask to be referred to a cardiologist or a lipidologist- they specialize in Cholesterol management.
Hmm this sounds like a good idea. Are they much more up to date in the latest research and studies?
They are supposed to be the experts in the treatment of high cholesterol. Try a university hospital, if possible or a large community hospital…
1 Like
An acquaintance of mine has been a practicing lipidologist for many year and has a subscription to The Skeptical Cardiologist. I’ve checked it out and am very impressed at the logical and practical advice given there.
Here’s the latest on statin decision making utilizing a combination of the CAC score along with an advanced risk calculator.
2 Likes
This is a very good approach for people over 60. At that age, I would give a CAC of 0 a lot more weight.
For people under 60 and that generally look healthy, I think that looking at plaque buildup in the femoral artery is even more useful than CAC.
And as we know, 10 year risk scores are literally useless for people under 40.
2 Likes
If you think it’s a good approach, just know you are basing your decision on epidemiological cohort studies.
rivasp12, thank you for the lead.
I just subscribed to the Skeptical Cardiologist.
2 Likes
Yep, I’m aware. You could do far worse
I don’t think that makes it any better.
I used to do exactly this. Then I discovered independent risk variables.
5 Likes
I don’t agree with the idea that all the evidence points towards “the lower the better” for LDL. At least not if we are talking about all-cause mortality. However, it is accurate if we are talking about CVD. The lower the LDL, the lower the risk of CVD.
I say this as someone who takes both a rosuvastatin and ezetimibe. In my case, CVD risks are high and lowering them are likely to benefit me.
But for others with more normal CVD risk, lowering LDL may be contraindicated if the goal is to live. If the goal is to not die of CVD, sure, take a statin.
There is a good paper with the title “Association between low density lipoprotein and all cause and cause specific mortality in Denmark: prospective cohort study” [BMJ 2020;371:m4266 http://dx.doi.org/10.1136/bmj.m4266]
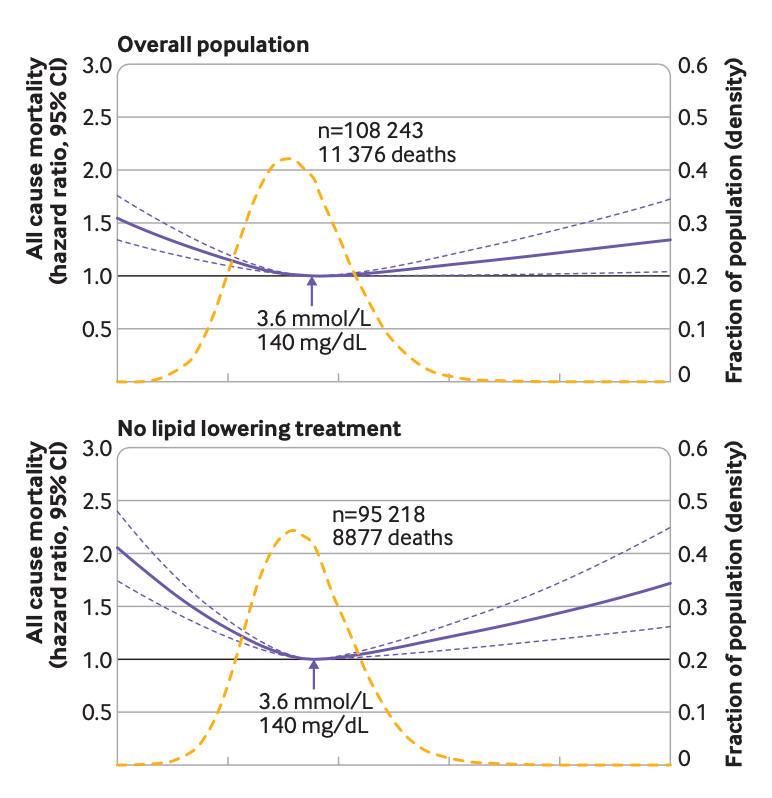
My personal conclusion is that for people with LDL around 140 mg/dL, unless they have very high risk factors for CVD, may actually not benefit from a statin and possibly may be harmed.
3 Likes
Just FYI, it has been studied many times and always been shown that the group of people who reliably comply with medication prescriptions do better than those who don’t. These two groups of people are different in many ways, basically.
This can be thought of as an element of the ‘healthy user bias’.
So there are two effects in this type of observational work: (1) we are measuring the impact of the drug provided and taken consistently, and (2) we are measuring the differences in outcomes between these groups. It is nearly impossible to disentangle these two effects.
Ultimately we don’t know if any of the signal we are measuring is due to item (1) versus (2).
In theory you could assign many people a placebo over many years and see what happens to the group that reliably takes it. We know that group will do better than the group that doesn’t.
I am unaware of any high-quality RCTs on statins with all-cause mortality as an outcome. I am personally convinced that for some people, including me, they are very helpful. Accordingly, I take one. But I am not convinced they are right for everyone.
Does the study say what these people died from?
My original comments were from about 1 year ago. I no longer take a statin because it does not appear to be particularly beneficial to people my age. Though the one study I cited says:
" The protective effect of statins observed among the very old appears to be independent of TC."
1 Like
There’s no known harm from lowering LDL as far as you can get it (unless the harm is from a non-cholesterol-related side effect of a medication, if that’s the treatment under consideration). The kind of correlational LDL/mortality study you mention has been previously discussed in this thread. These studies are not helpful because of (among other reasons) the fact that by definition they don’t establish cause-effect and because of a “sick patient” bias (sick people who die earlier often have lower LDL as a result of their illness, and they skew the results).
Of course, this is not to say that “everyone should be on a statin” (that’s a straw man which continues to be abused ad nauseum), but since CVD is the #1 leading cause of death, it makes sense to me to keep LDL/ApoB as low as possible with diet first (free of potential side effects) and potentially meds/supplements second (after weighing potential benefits vs safety and cost).
4 Likes
I am a bit confused. How do I find my ApoB? I am looking at my last blood report and I only have cholesterol (TOTAL), LDL, Triglycerides, HDL, and cholesterol to HDL ratio.
The values are (in mg/dl):
TOTAL: 140.76
LDL: 81.2
Triglycerides: 57.62
HDL: 39.83
Ratio: 3.53
Is this good, bad, or ugly?
1 Like
Why are you on this site? What are you doing here?
2 Likes
Your mindset appears to be that lower LDL is always better in all contexts. But the epi study shows that may not always be true. Certainly, as you say, correlational work of that sort has its limits.
(Although the “sick patient” bias should not be a major confounder - that happens more if you are measuring LDL when people arrive at the hospital; these measurements are years before death in most cases. But nevertheless, we can’t say for sure - agreed.)
But can’t say for sure is true in both directions - we can’t say that lower LDL is helpful in all contexts. We lack data.
You say that you aren’t saying that “everyone should be on a statin.” But when I read everything you write - with the exception of that sentence - it seems like your logic dictates that they should be. Probably this is just due to my misunderstanding. But I guess it would clarify your position if you mentioned a few examples where you don’t believe a person should be on a statin.
1 Like