It’s the “may” that we’re trying to discern. You can find dozens of papers and studies supporting higher LDL, TC in older cohorts and longevity. Sounds like confirmation bias.
But where are the facts Rapamycin induced lipids dsyregulation is benevolent?
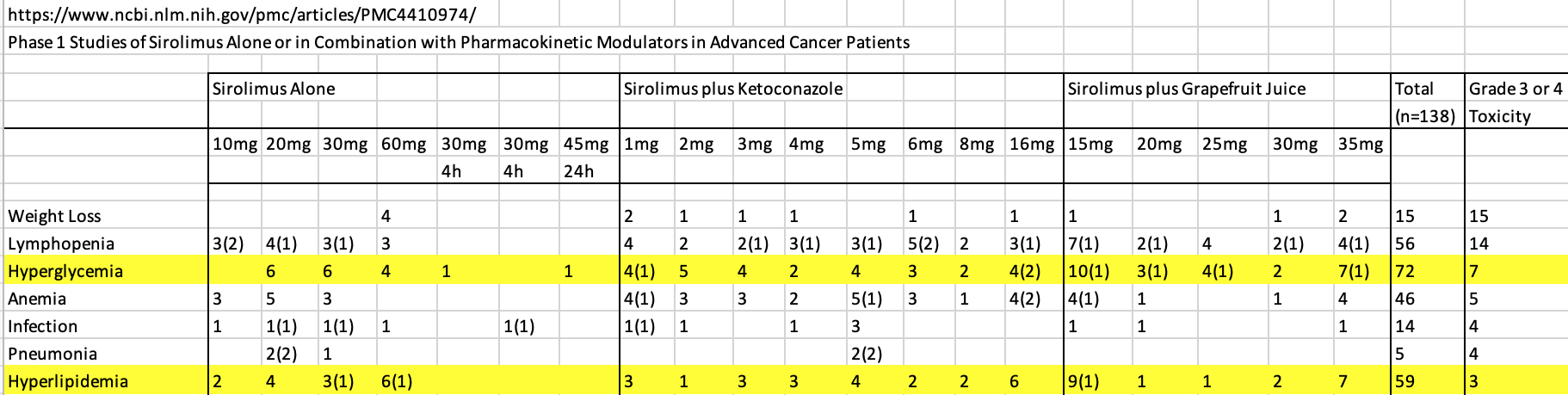
How many of these “LDL/TC type” studies look under the hood at the true underlying risk factors like apoB, sdLDL, ox-LDL, CAC progression rate and 10yr CVD risk? Or an even more in depth cardio risk profiling offered by the Cleveland Heart Clinic.
I don’t recall they looked at these metrics for the wild type ITP mice? So the takeaway: Rapamycin increases longevity, translatable to humans, happily accept the cause of death.
However for us humans who can get neurological diseases late in life, I certainly don’t want to get AD at normal epidemiological age, and be kept alive (and be a longevity statistic) ONLY because of the physical reserve benefits conferred by Rapamycin? That’s not a tradeoff for me. I want AD pushed out by Rapamycin. I’d like to know if Rapamycin increases my risk odds, either by some core neurological pathway mechanism (eg. TREM2) OR via dysfunctional cerebral cause by peripheral intervention.
Why do the studies showing cardiovascular benefits or Rapamycin administration in mice have to resort to such dsyfunctional, transgenic mutant, genetic fantasy compromised mice?
mTOR drives cerebral blood flow and memory deficits in LDLR (-/-) mice modelling atherosclerosis and vascular cognitive impairment
Cardioprotective effects of dietary rapamycin on adult female C57BLKS/J-Leprdb mice
So I went back at looked at one of the early seminal Rapamycin/mice/longevity studies in wild type mice.
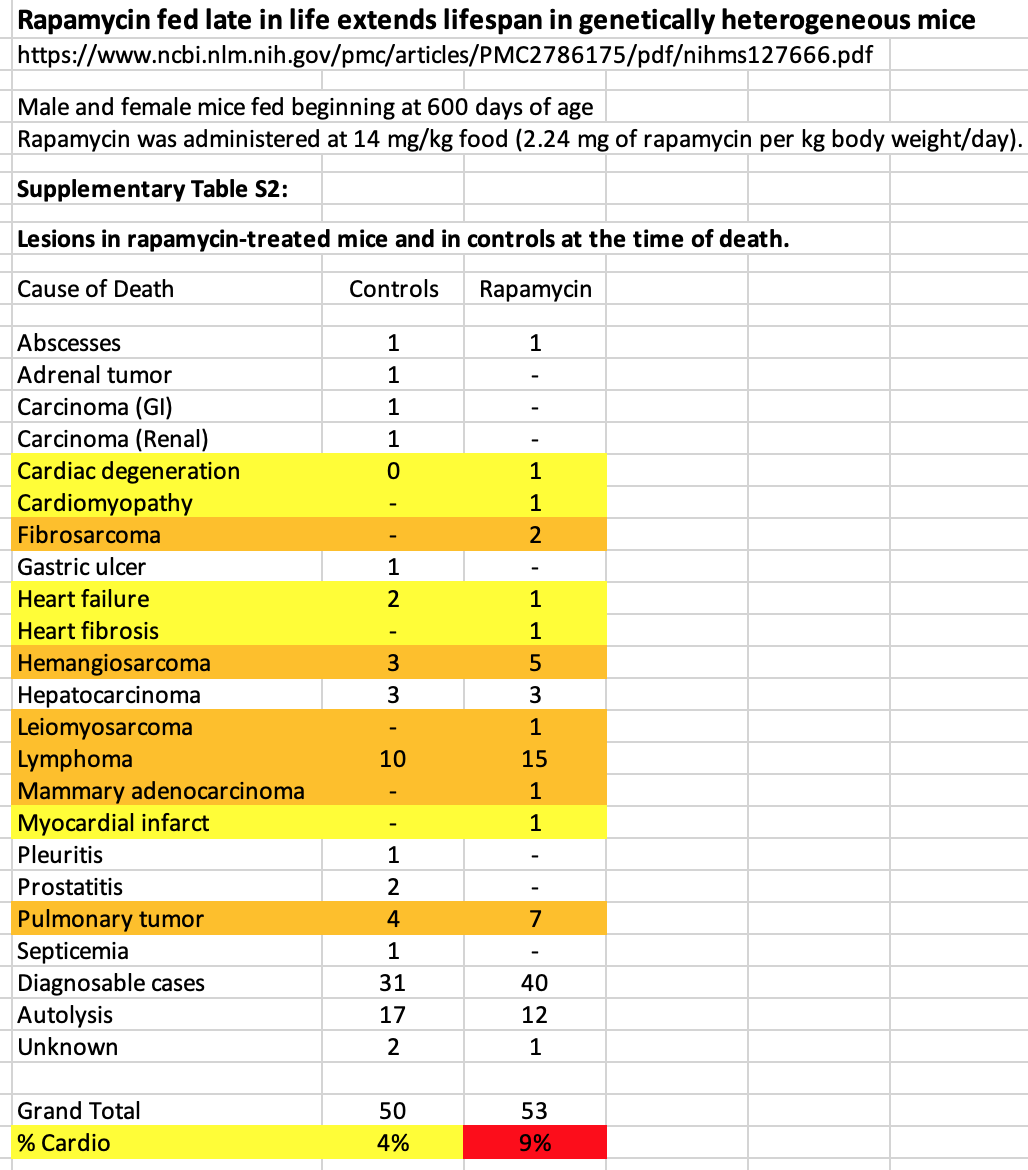
Rapamycin fed late in life extends lifespan in genetically heterogeneous mice (2009, Richard Miller)
I dug out the supplementary data where they reported on pathological cause of death.
Herein. As expected, cancer related represents 90% of deaths in both control and Rapamycin, but sub group analysis shows cardio related deaths DOUBLE IN THE RAPAMYCIN COHORT?!
Not only that, certain types of caners are higher in the Rapamycin cohort (Fibrosarcoma, *Hemangiosarcoma, Lymphoma, Pulmonary Tumour) showed higher prevalence than in control mice?
*Hemangiosarcoma (Hemangiosarcoma - Wikipedia) Hemangiosarcoma is a rapidly growing, highly invasive variety of cancer arising from the lining of blood vessels; that is, blood-filled channels and spaces are commonly observed microscopically. Sounds nasty.
Yes, ok, they lived longer on Rapamycin, but dosen’t sound cardio benevolent (nor pan cancer benevolent) to me for these wild type mice. Of course, we’re talking MICE and CHRONIC Rapamycin administration. But these wild type mice don’t have metabolic syndrome or are sedentary I might add, and this could be a significant confounder in human translation.
The higher prevalence of cardio related causes of death in these mice didn’t happen on the last day of their lives…they likely slowly manifested, just like in humans. So some interesting dynamics at play re Rapamycin initiating more cardio related degenerative pathways, yet still pushing their mortality outcome to later in life?
So, this would reinforce the point of MEASURING (deep lipid panel, CAC) your true risk dynamic whilst taking Rapamycin.
My point…this is an unresolved issue in human interventions.