Interesting. Thx for the perspective.
My end goal is better functioning cells. I think the reason people use Yamanka factors is the concept of resetting a program of aging (like rebooting a computer). I don’t think that’s how aging works.
My ApoB has been as low as 77mg/dl and normally bounces around the 90 mark. The last measurement was 92.
How much of aging do you think your approach will cover (or solve)? I think there must be more things than just a shortage of acetyl-CoA, if I am understanding it correctly. 90 is around 50th percentile, but ASCVD is normal thing happening to people in the 50th percentile.
I am working on two cellular functions. One relates to acetyl-CoA levels in the nucleus and is the issue of aberrant splicing and transcription failures. The other relates to mitochondrial efficiency and the provision of ATP to the Ribosome. In the former case the wrong mRNA is produced and in the latter case the proteins are not produced and sent off to Ribosome Qualty Control for recycling.
I think these are the major causes of the phenotypes of aging and also those cancers relating to aberrant splicing (I don’t know what proportion this is). I count metabolic syndrome as a phenotype of aging.
There are other stochastic elements and obviously there is some DNA damage that occurs that this does not fix.
Allocating any numbers to this is hard, however. My personal view is to fix this and then see what happens.
There was an experiment with citrate and drosophila
I think they got the mechanism wrong.
2 Likes
John, how are you dosing the citrate?
Which type/ types?
Are you measuring systemically?
1 Like
FWIW
Located the following;
Swanson Ultra
Retail Cost under $6.00 per 60 capsules
Cost $2.79 per 60 capsules bottle on 11/26/2023
Mineral Citrate Complex - Calcium, Magnesium, Zinc, Potassium
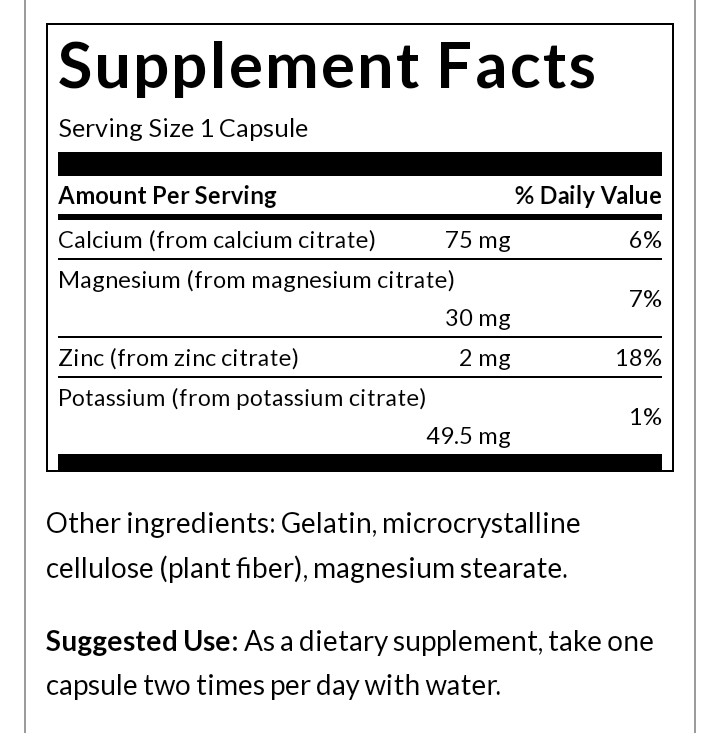
On a practical basis it is better to ask questions on the protocol thread. However, those masses are the cation masses. I would guess that there is perhaps 400mg of citrate in each capsule.
“However, the exact mechanisms of action of citrates have never been accurately described and results obtained so far often failed to demonstrate a significant advantage”
Is this true?
They are part of the AKG cycle but besides that there’s no real evidence it does anything for longevity.
My work on citrates started in 2022. I think it works for me. Only a few people have tried it, mainly friends and family. It seems worth a try, but people have to be careful and i dont promise anything.
1 Like
I dont think anyone else is studying it the way i am.
It seems that the drug interaction between ezetimibe snd gemfibrozil is minor. The most important interaction seems to be an increased risk of developing gall stones if supplementing for a long time. I plan to take both and not do gemfibrozil permanently.
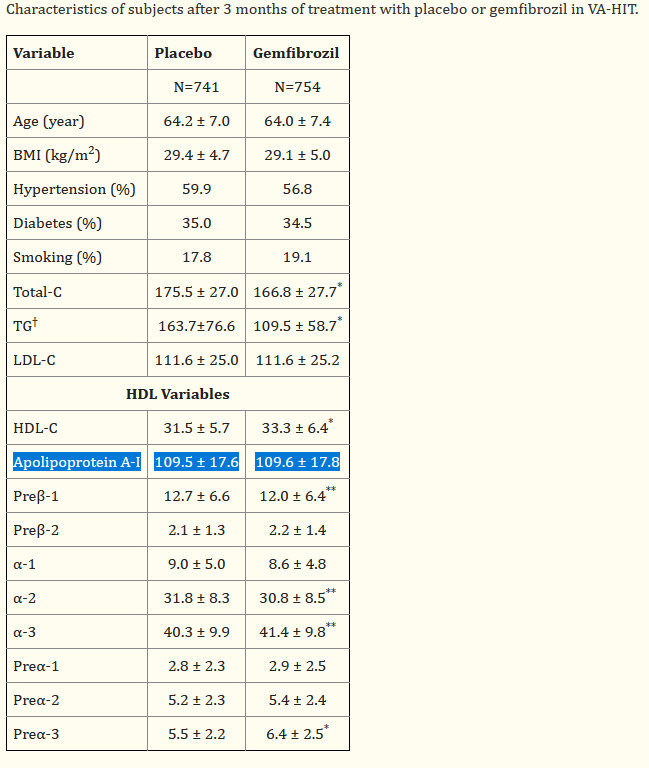
There is a tendency for gemfibrozil to increase plasma concentration of ezetimibe:
Objective: Ezetimibe is a novel lipid-lowering drug that prevents intestinal absorption of dietary and biliary cholesterol leading to significant reduction in total-C, LDL-C, Apo B, and TG and increases in HDL-C in patients with hypercholesterolemia. Gemfibrozil, a fibric acid derivative, is an effective lipid-modulating agent that increases serum high-density lipoprotein cholesterol and decreases serum TG. The objective of this study was to evaluate the potential for a pharmacokinetic (PK) interaction between ezetimibe and gemfibrozil.
Methods: This was a randomized, open-label, 3-way crossover, multiple-dose study in 12 healthy adult male volunteers. All subjects received the following 3 treatments orally for 7 days: ezetimibe 10 mg once daily, gemfibrozil 600 mg every 12 hours, and ezetimibe 10 mg once daily plus gemfibrozil 600 mg every 12 hours. A washout period of > or = 7 days separated the 3 treatments. In each treatment, blood samples were collected on day 7 to assess the steady-state PK of ezetimibe and gemfibrozil. The oral bioavailability of ezetimibe coadministered with gemfibrozil relative to each drug administered alone was evaluated with an analysis-of-variance model.
Results: Ezetimibe was rapidly absorbed and extensively conjugated to its glucuronide metabolite. Ezetimibe did not alter the bioavailability (based on AUC) of gemfibrozil. The mean AUC0-12 of gemfibrozil was 74.7 and 74.1 microg h/ml with and without ezetimibe coadministration, respectively (log-transformed geometric mean ratio (GMR) = 99.2; 90% confidence interval (CI) = 92 - 107%). Conversely, gemfibrozil significantly (p < 0.05) increased the plasma concentrations of ezetimibe and total ezetimibe (i.e. ezetimibe plus ezetimibe-glucuronide). Exposure to ezetimibe and total ezetimibe was increased approximately 1.4-fold and 1.7-fold, respectively (CI = 109 - 173% for ezetimibe and 142 - 190% for total ezetimibe), however, this increase was not considered to be clinically relevant. Ezetimibe and gemfibrozil administered alone or concomitantly for 7 days was well tolerated.
Conclusions: The coadministration of ezetimibe and gemfibrozil in patients is unlikely to cause a clinically significant drug interaction. The coadministration of these agents is a promising approach for patients with mixed dyslipidemia. Additional clinical studies are warranted.
May I asked what the benefit part of the rationale is for a temporary dosing is?
The uncertainty, and the mixed opinions whether there is an interaction concerns me, as that is not typical for other drugs I take or want to take, hence I will avoid it as it doesn’t seem to increase apoA1 which I was looking for, for Alzheimer’s.
Bezafibrate? Post must be at least 20 characters
I have not looked at apoA1 increasing drugs or supplement (or even food) space. So I don’t know what to compare it with. Do you know? I wonder if I could get a chemical synthesis of a CETP inhibitor… ![]()
There is one therapy, called lipoprotein apheresis, that involves removing Lp(a) from the blood using IVs.
1 Like
Discussed a bit more here
And here
1 Like
This is quite interesting though. A 5 year old S Korean study showing a positive result.
‘For the blood lipid profile, the policosanol 10 mg and 20 mg groups showed significant reductions in total cholesterol (TC) of around 8% (p = 0.029) and 13% (p = 0.0004), respectively, at week 24 compared with week 0. Serum HDL-C level significantly increased up to 16% and 12% in the policosanol 10 mg (p = 0.002) and 20 mg (p = 0.035) group, respectively. The study results suggest that long-term policosanol consumption simultaneously reduces peripheral BP as well as aortic BP accompanied by elevation of HDL-C and % HDL-C in TC in a dose-dependent manner.’
1 Like