The age standardized death rate from cancer has slowly declined over the past 20+ years.
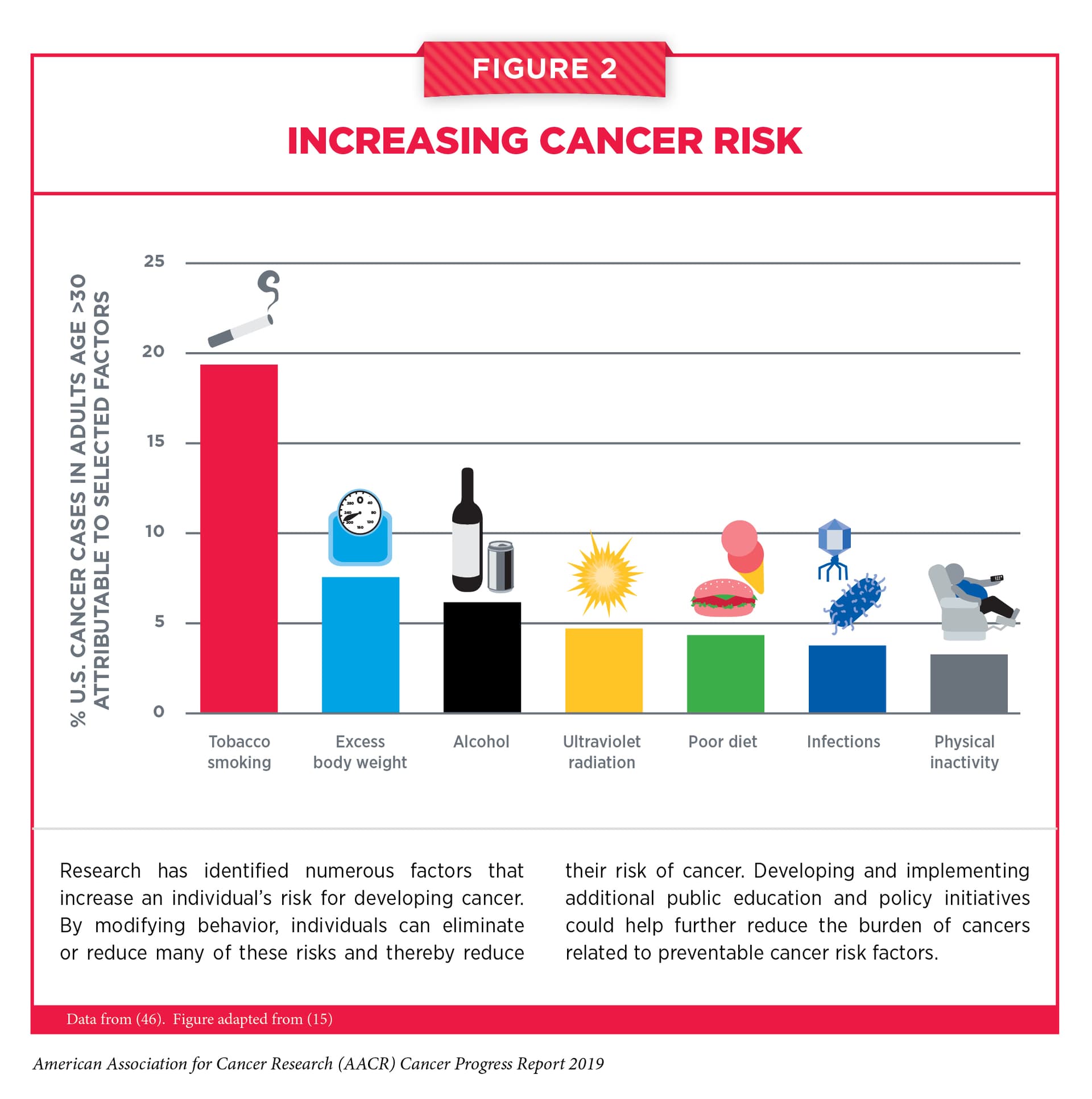
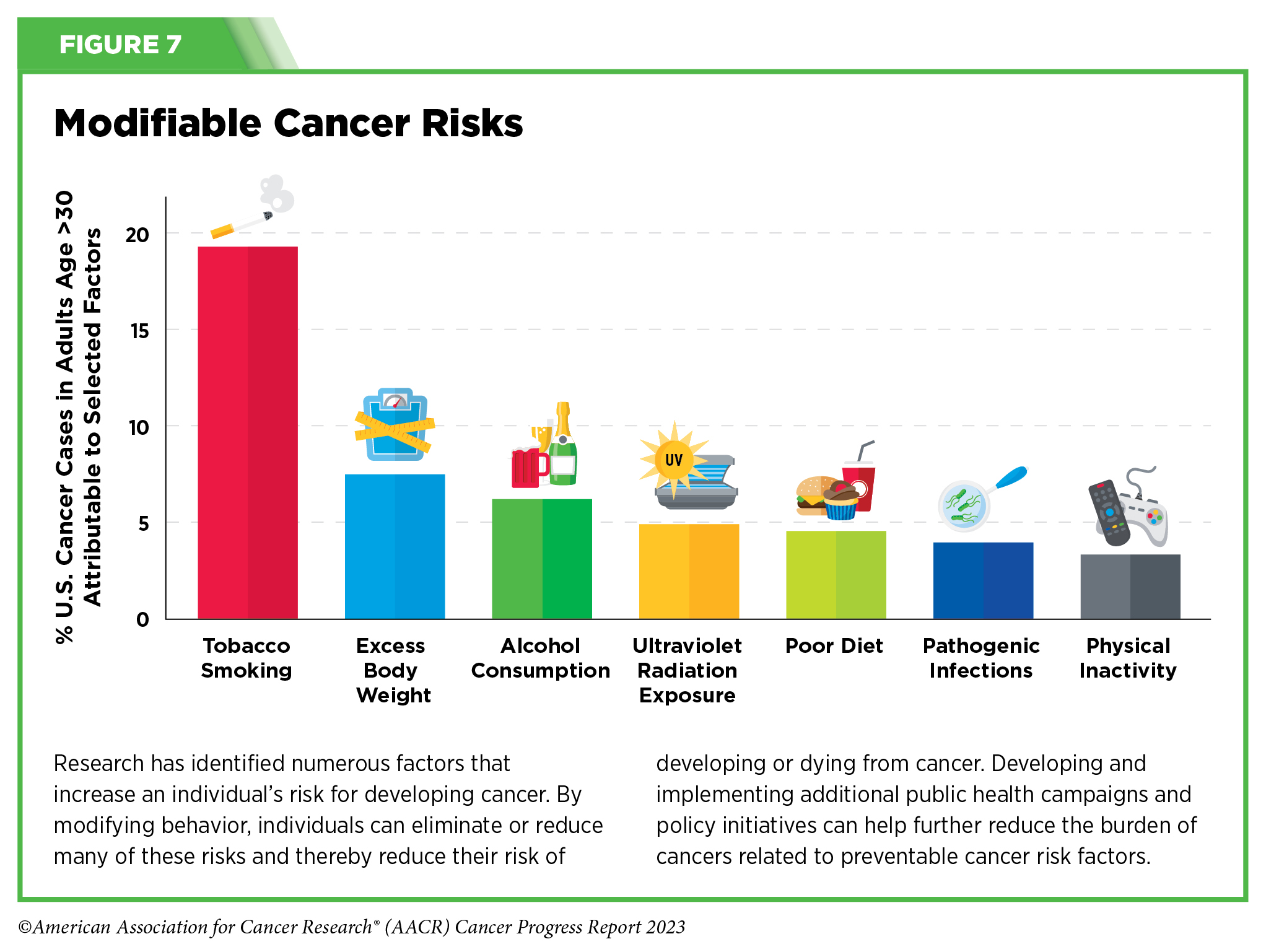
20% of cancer are attributed to smoking in high income countries. Other modifiable risk factors are obesity, alcohol, sun exposure, diet, infections and physical activity:
I think Thomas Seyfried’s work on cancer needs more attention.
His argument is that cancer is substantially metabolically driven in that the mitochondria don’t work properly and the cell starts relying on fermentation for energy rather than OxPhos.
IMO this would lead to limitations on acetylation and as a consequence aberrant splcing and it may be the aberrant splicing that leads to the conclusion that there are genetic problems.
It is clear for prostate cancer that aberrrant splicing (producing the wrong protein from only part of the gene) is a major part of the problem.
I would be interesting in seeing PSA results from citrate supplementation other than my own. Most of the time my PSA figures (for a 64 year old man) are below 1 (off the top of my head micrograms per litre). Interestingly they shot up to 4 recently then over a period of weeks came back down below one.
Because of the prostate’s role in injecting citrate into seminal fluid I think citrate is particularly important when it comes to the prostate. However, the only test results I have on this are my own.
So combined with the 50% modifiable risk factors that’s already a massive reduction.
However, reading the paper I don’t understand how often they modeled the test would be used. The test costs $1k but let’s imagine competition joins the market and the price goes down to $100. If, theoretically, you get tested very year, could you totally eliminate your risk of cancer death by nipping in the bud any new cancer at a very early stage?
I am not up-to-date on the latest whole-body MRI techniques, their usefulness, or what is known about whole body MRI and its role in early detection. But the hive mind here has the experience and the knowledge. So it can be good to have this focus at the beginning of the thread.
Then there are the roles of more specific screenings, like mammograms, and colonoscopies. Tools better suited for specific cancers?
Contrary to many naysayers, PSA is a valuable tool. Is it perfect, of course not, it has distinct limitations. But, for us older men (currently I’m 66), here’s one study from Sweden that I think is very useful:
Basically, if by age 60, your PSA is at or below 1ng/ml, your chances of dying from PC by 85 is minimal.
However, we need to keep in mind that the PSA number is affected by many factors which distort it. For example, statins tend to lower the PSA number, so that may give you a false sense of security, so for risk evaluation you need to adjust for that.
My thoughts:
I hate “5 year survival”. Especially when it gets correlated with “cure”. I’ve known countless people who died from their cancer in year 6 or 7.
I think it’s overly optimistic to think we can reduce our risk by 50% by behavior. There is a lot of overlap, rather than separate risk to each behavior, and some of it is correlation rather than causation.
It’s way too simplistic to think cancer has a common mechanism. It will take multiple different treatments individualized to specific cancer types to treat and cure.
At our current level of treatment, early detection is huge. Unfortunately, we don’t have diagnostic methods yet for many cancers to detect early enough.
The 5y period is useful to standardize. Then you can use compounding to get the survival over a longer period of time. For instance 75% 5y survival rate would imply only 56% over 10y. That’s why we need to get to 95% 5y survival, which would imply 90% over 10y and 81% over 20y.
An estimated 40% of all cancer cases and nearly one half of all cancer deaths in the United States in 2019 were attributable to the evaluated potentially modifiable risk factors. These findings reinforce that the morbidity and premature mortality from cancer in the United States can be substantially reduced through broad and equitable implementation of known preventive initiatives, such as excise taxes on cigarettes to reduce smoking, screening for and treating HCV infection, and vaccination against HPV infection.
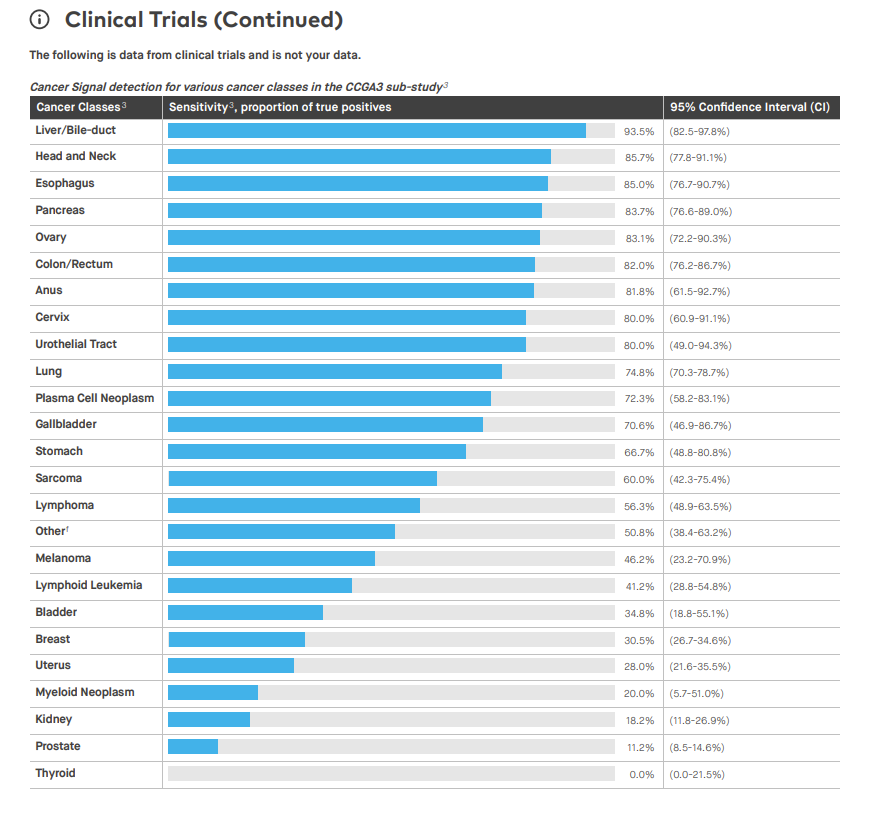
Less aggressive cancers, such as many thyroid cancers, release less cell-free DNA into the bloodstream and are less likely to be detected. More aggressive cancers, such as pancreatic cancer, tend to release more cell-free DNA into the bloodstream at early stages and are more likely to be detected. Higher Galleri sensitivity for the deadliest cancers helps minimize overdiagnosis and/or overtreatment of indolent cancers. Galleri has high sensitivity (76.3%) for 12 deadly cancers that comprise two-thirds of all cancer deaths, and an overall sensitivity of 51.5% for all cancers and across all stages.
What I wonder is: if you do Galleri (or TruCheck or whatever) every year, how much do you lower your lifetime risk of cancer death? I can’t find any data on this besides “The Galleri test could result in a 26% reduction in 5-year cancer-related mortality when added to usual care (based on modeled data)”.
GRAIL’s primary advantages would appear to be large financial resources (the company has raised over $2 billion in private capital) and political influence, with former UK Prime Minister David Cameron consulting for parent firm Illumina, and the CEO of GRAIL Europe being Harpal Kumar, former Chief Executive of Cancer Research UK and member of the UK Research and Innovation Board. What role might these advantages have played in the selection of the Galleri test for evaluation in the NHS, when rival technologies are available?
“All screening programmes do harm; some do good as well, and, of these, some do more good than harm at reasonable cost.” A cancer screening programme that offers no improvement in cause-specific mortality (or quality of life) is only doing harm and wasting money. The GRAIL-Galleri trial must, as a minimum, show direct benefit in reducing cancer-specific mortality. This observation should feed into an independent, scientifically valid evaluation as is standard for other new candidate cancer screening programmes. Although commercial interests are powerful, world-firsts are politically attractive and patient groups champion screening for their cancer type, the NHS can ill-afford to be a world leader in the adoption of poorly evaluated interventions that might be of little or no benefit, harm people, and waste resources that could be better used elsewhere.
The NHS-Galleri trial was designed with three consecutive years of screening, and it is vital to evaluate the primary objective and endpoints at the end of the study in 2026. The primary endpoint of the trial is an absolute reduction in the number of late stage (stage 3 and 4) cancers diagnosed, and cancer-specific mortality will also be analysed after five years of follow up.
So we’ll only know in 2031 if Galleri reduces 5y mortality…
I had the Galleri test a couple of years ago shortly after it came out ($1K). I tested “positive” or “elevated” for breast cancer (very highly elevated) and prostate cancer (very low).
The low cancer “bar” was not shocking. Several close male relatives over the years have had prostate “cancer”, but none of them died of it. It is “indolent”, which my wife didn’t know the definition of, and she laughed when I told her it basically meant “lazy” or a “lay-about”. So my male relatives make it into their 80’s and even 90’s and the cancer never acts up and they end up generally dying of cardiovascular disease. I talked with my PCP and he said to get an exam every couple of years and if the yearly blood test of PSA was not elevated and if I was peeing OK, then the “do-nothing” approach works just fine, which was OK by me.
But the breast cancer high bar was weird. Still, I took a mammogram and several other tests but bupkis, nothing, as I expected. About 500 men in the U.S. die of breast cancer every year, so it’s a real thing, but not very likely.
I think the company “dials the cycle#” way high for breast cancer because they really really don’t want to miss a case, especially when they were first coming out a couple of years ago when they were trying to get approved/certified for more states. If they had “missed” a case, especially from a high-profile person, it would have wrecked their chance of full approval and/or acceptance. So from their viewpoint, it’s far better to vastly over-diagnose and have 10% or even more of male patients experience (and pay) for mammograms.
So I wasn’t impressed by it. In my case, the early version was useless, imho.
What about full body MRI for cancer prevention @DrFraser@KarlT? Besides the cost, do they suffer from the same issue as Galleri (low sensitivity and many false positives)? As cancer grows quickly, do you need to do it yearly for it to be useful? Will the technology improve?
I’m recommending whole body plus MRI’s from SimonOne to most of my patients over 50 years. As a screening for vascular disease, having an MRA of the neck and head is pretty valuable, so I know how worried to be about their lipids and how tightly to manage them. Someone who is 75 years old and has not a bit of plaque in their carotids, no small vessel disease in their brain, nothing we see in their aorta … I’m pretty happy not being less aggressive on lipid management.
They also provide Neuroquant and tell you %tile of your hippocampus for example.
You’ll know if you have brain atrophy.
It’s important with the MRI’s and other imaging to not do invasive diagnostics, unless something is truly concerning. Not every abnormality requires investigation. This is where working with an experienced physician is helpful, as most of the time, abnormalities simply get tracked on yearly MRI and not investigated.
For the cancer screening on blood, I’ve gone to the product TruDiagnostic has, as it looks better than Galleri - I don’t routinely pursue that due to risk of results I’m not sure what to do with … probably happier just sticking with the MRI right now.
I would say it’s of use if you are looking for something specific. If you are just scanning to look for anything worrisome then the problem of false positives arises. My experience has been that if you look enough, you will find something, but often it’s not anything of concern but it has to be evaluated which can be expensive and with possible adverse events.
Historically, parous women – women who have given birth – were known to be less likely to develop breast cancer than nulliparous women – women who have never given birth. This protective effect of pregnancy reduces the risk of developing a type of breast cancer called estrogen receptor-positive tumor.