Nine trials enrolling 35 222 patients were included in the analyses. Compared with the control group, ezetimibe increased the number of new intestine cancer patients [relative risk (RR), 1.30; 95% confidence interval (CI), 1.02–1.67; P = 0.03] and had a trend to increase the number of new breast cancer patients (RR, 1.39; 95% CI, 0.98–1.98; P = 0.07). There was no significant difference in new hepatobiliary cancer, prostate cancer, skin cancer or cancer of other sites. Ezetimibe did not significantly increase the risk of new cancer in total (RR, 1.03; 95% CI, 0.96–1.11; P = 0.38), cancer-related death (RR, 1.11; 95% CI, 0.98–1.26; P = 0.10) or cancer events (RR, 1.04; 95% CI, 0.97–1.12; P = 0.30). In terms of lipid-lowering effect, ezetimibe significantly reduced total cholesterol and low-density lipoprotein cholesterol, increased high-density lipoprotein cholesterol.
Maybe this whole model, where healthy people take medications intended for diseases, is flawed. Perhaps all medications have some drawbacks, meaning they increase the risk of some cancer or other illness. Now, if you’re healthy and don’t know your personal genetic risk factors, you might do more harm than good. The situation is much more clear when it’s known that there’s a significantly high risk of a certain disease. This is just a thought.
What do you call “healthy” and “disease” here? I mean: from which levels of ApoB (or whatever other marker) do you consider someone to have a “disease” and not being “healthy”?
I mean the actual clinical recommendations for the use of medications.The comment was made on a general level, not specifically directed at Ezetimibe. I use it myself, but on the other hand, I have a known elevated genetic risk for cardiovascular diseases.
I use few medications for which there are no clinical indications, but I have often thought about what I wrote.
New generation of cancer-preventing vaccines could wipe out tumors before they form
Shots enter early clinical trials for healthy people at high risk for disease
When Dave Dubin learned at age 29 that he had colon cancer, it wasn’t a big surprise. His grandfather and father had both survived the disease. “It was almost the Dubin way, and we just went on,” Dubin says. He had surgery and chemotherapy, but his cancer came back 10 years later. Genetic testing finally found an explanation for his family’s trials: a mutation in a DNA repair gene that lets genetic errors pile up in dividing cells. The disease, Lynch syndrome, comes with up to a 70% lifetime risk of cancer.
Dubin, 55, gets annual colonoscopies, endoscopies, and imaging scans, which caught a third cancer, in his kidney. His eldest son, Zach Dubin, 26, inherited the DNA repair mutation and also regularly gets checked for cancer. “It’s no fun. Nobody enjoys it,” Dave Dubin says—not the 2-day colonoscopy prep and procedure, nor the worrying about possible tumors. The disease also turned him into an activist. He and his family in Haworth, New Jersey, launched a nonprofit, AliveAndKickn, to promote research and awareness of Lynch syndrome, which affects an estimated 1.1 million people in the United States.
…
Vaccines to prevent certain types of cancer already exist. They target viruses: hepatitis B virus, which can trigger liver cancer, and human papillomavirus, which causes cervical and some other cancers. But most cancers are not caused by viruses. The Lynch vaccine trial will be one of the first clinical tests of a vaccine to prevent nonviral cancers.
The idea is to deliver into the body bits of proteins, or antigens, from cancer cells to stimulate the immune system to attack any incipient tumors. The concept isn’t new, and it has faced skepticism.
I find this interesting as I know people who have had a stroke and then get diagnosed with cancer a few years later…
Epigenetic age and long-term cancer risk following a stroke
Background
The association between increased cancer risk following a cerebrovascular event (CVE) has been previously reported. We hypothesize that biological age (B-age) acceleration is involved in this association. Our study aims to examine B-age as a novel contributing factor to cancer development post-CVE.
Conclusions
Our findings suggest that epigenetic accelerated aging, as indicated by Hannum’s EEAA, may play a significant role in the increased cancer risk observed in CVE survivors.
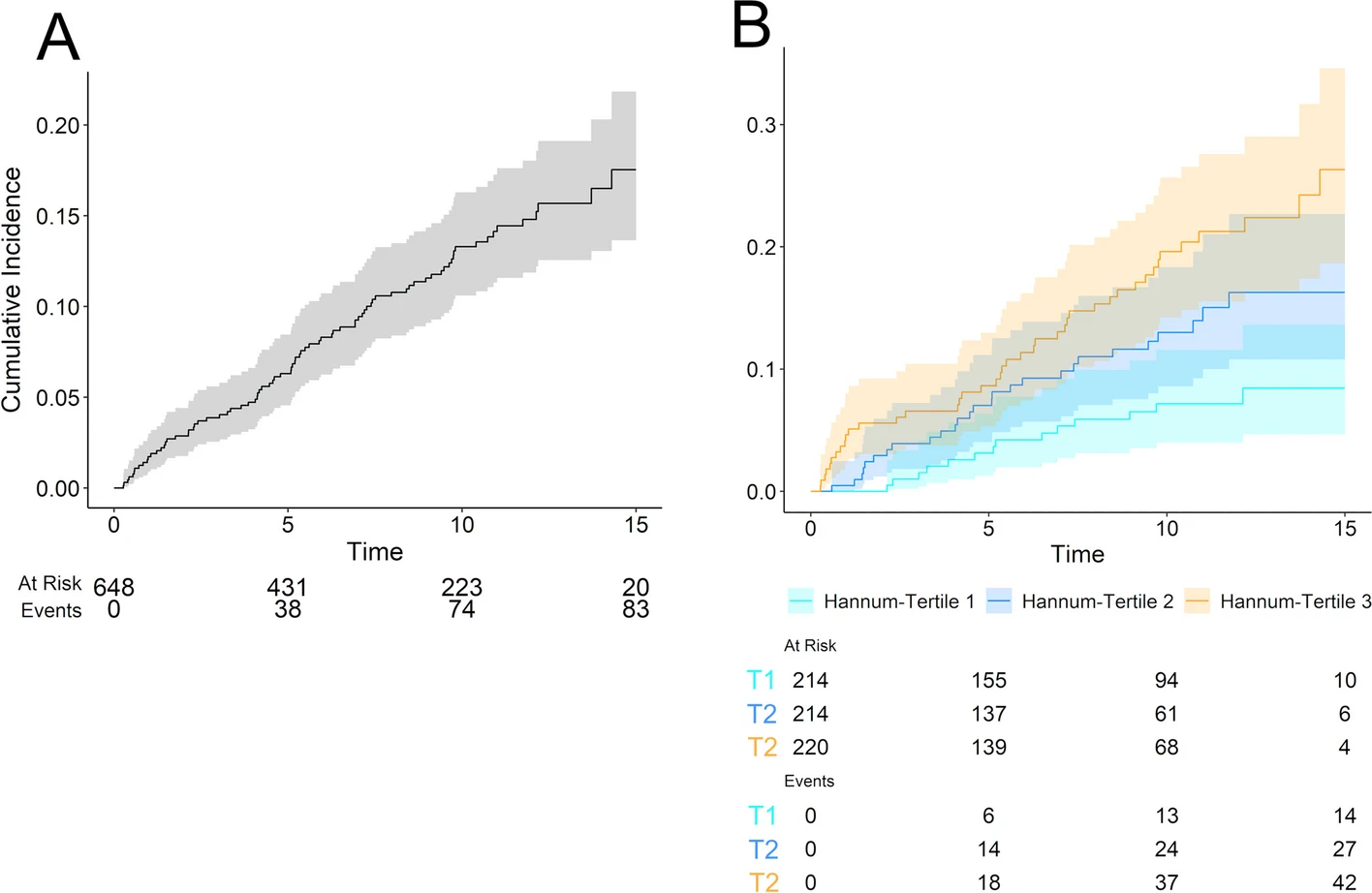
Cumulative incidence of cancer in the cohort. Values represent the number of patients at risk and the cumulative number of events. A shows the cumulative incidence function in the whole sample, while in B we stratified the incidence by tertile-split Hannum extrinsic epigenetic age acceleration. Time is represented in years. T1, first tertile; T2, second tertile; T3, third tertile
Is it a good journal? The first thing I think about if they got a significant result simply by random chance (after all if you test for 30 cancers, one will be significant to such a degree), but they should’ve corrected for this.
Called the Acid King by the media,[3][4] Stanley was the first known private individual to manufacture mass quantities of LSD.[5][6][7] By his own account, between 1965 and 1967, Stanley produced at least 500 grams of LSD, amounting to a little more than five million doses.[8]
Owsley is in the The Sunshine Makers (2015) documentary I think and which explains all of this for those who weren’t from that era or even consumed (maybe @Steve_Combi was a part of it).
I took a small dose of LSD when I was 20, I think I found that good.
It’s a good reason for me to stop it! Was taking half pill for a few months. Noticed occasional nausea in the morning after I take it. Done with ezetimibe!
Dozens of studies prove the benefits of ezetimibe. The cancer risk comes from a single paper by a traditional Chinese medicine research group (). Until proven otherwise, the risk/benefit ratio seems clear and massive in favor of ezetimibe.