Does α-Amyrin Boost Autophagy, Thwart Tau Pathology?
People who consume copious fruits and vegetables tend to enjoy healthier, longer lives, and are less prone to dementia. How could noshing on plants ward off age-related diseases such as Alzheimer’s? According to a paper published on January 22 in Advanced Science, a bittersweet molecule called α-amyrin might be part of the answer. Found in numerous common fruits, including cranberries, pears, bell peppers, eggplants, tomatoes, grapes, cherries, passion fruits, and olives, this triterpenoid reportedly thwarts tau aggregation in cell culture and in mice. Led by Patricia Boya of the University of Fribourg, Switzerland, Tewin Tencomnao of Chulalongkorn University in Bangkok, and Evandro Fei Fang of the University of Oslo in Norway, the authors report that α-amyrin works its magic by stimulating mitophagy, boosting mitochondrial health and clearance of aggregated proteins. In a parallel, the scientists found that people who consumed high amounts of fruits and vegetables not only had a lower risk of dementia, but a hint of less p-tau217 in their blood. That it readily crosses the blood-brain barrier makes α-amyrin a therapeutic candidate, the authors contend.
Because α-amyrin survives for hours in the plasma and can cross the blood-brain barrier in mice, the authors are planning to test it in people. Fang told Alzforum that since pure α-amyrin is expensive, his group is working with industry partners to synthesize it. He did not know how many passion fruits a person would need to eat to benefit, but noted that his lab has detected α-amyrin in the skin and seeds, as opposed to the flesh. This distribution has been reported for other fruits, such as apples and tomatoes, as well (Brendolise et al., 2011; Bauer et al., 2004). Catalogued information about its concentration is not available, Fang told Alzforum. For now, he recommends that people simply add more colorful fruits and vegetables to their daily diet.
Alzheimer’s may start with inflammation in the skin, lungs or gut
The Alzheimer’s field is being turned on its head as mounting evidence points to the disease beginning outside the brain many years before symptoms start. This may mean we have to totally rethink how we approach preventing and treating the condition
To explore the genetic underpinnings of Alzheimer’s disease, Cesar Cunha at the Novo Nordisk Foundation Center for Basic Metabolic Research in Denmark and his colleagues studied genetic data from more than 85,000 people with the condition and 485,000 people without it from the European Alzheimer and Dementia Biobank. They also analysed gene activity in 5 million single cells from 40 areas of the body and 100 brain regions.
…
Intriguingly, the team found the highest expression of these gene variants when people were aged 55 to 60, suggesting that inflammation during this window is most likely to lead to Alzheimer’s disease. This is supported by a long-running study in Hawaii that found that men with raised markers of inflammation in their blood in their late 50s were more likely to develop the condition in their 70s and 80s. “You might get inflammation in your lungs from a viral infection when you’re 55, and that could translate to Alzheimer’s 30 years later. But we don’t know why yet, so there’s a very big piece in this whole puzzle that hasn’t been figured out,” says Cunha.
Rezanur Rahman at QIMR Berghofer Medical Research Institute in Australia and his colleagues also recently found that genetic variants associated with Alzheimer’s disease seem to cluster in the skin and lungs. But more work is required to prove that they do indeed play functional roles in the development of the condition, says Rahman. “Association does not mean causation.”
Blood test could predict dementia risk for women 25 years early
Less invasive than a brain scan, it can find high levels of a protein linked to a higher risk of developing dementia
A blood test could predict a woman’s chances of developing dementia up to 25 years before symptoms develop, scientists have claimed.
If a woman’s blood has elevated levels of a protein called p-tau217, which has been linked to the brain changes seen in Alzheimer’s disease, it could be a strong predictor for her risk of developing dementia decades down the line, a study has found.
The findings were gender-specific as the data was based on 2,766 participants in the Women’s Health Initiative Memory Study, which signed up women aged between 65 and 79 in the late 1990s and followed them for a quarter of a century. But the researchers said the protein is “strongly associated with dementia risk in men as well”.
None of the women had any cognitive impairments. Researchers from the University of California San Diego found that those women who had higher levels of p-tau217 at the start of the study were “much more likely to develop dementia later in life”.
The link was even stronger among those who had a higher genetic risk of Alzheimer’s, because they possess a genetic variant known as APOE-e4.
The blood test is less invasive than a brain scan or taking a sample of spinal fluid. However, blood tests are not currently recommended for people who are not yet showing any signs of cognitive impairment.
I think that seems very unfair - rather they are doing exactly what we want - funding science and clinical trials
This is the group that has done the most on showing the science and conducting placebo controlled clinical trials in humans
And it seems that the new funding is aimed at continuing that:
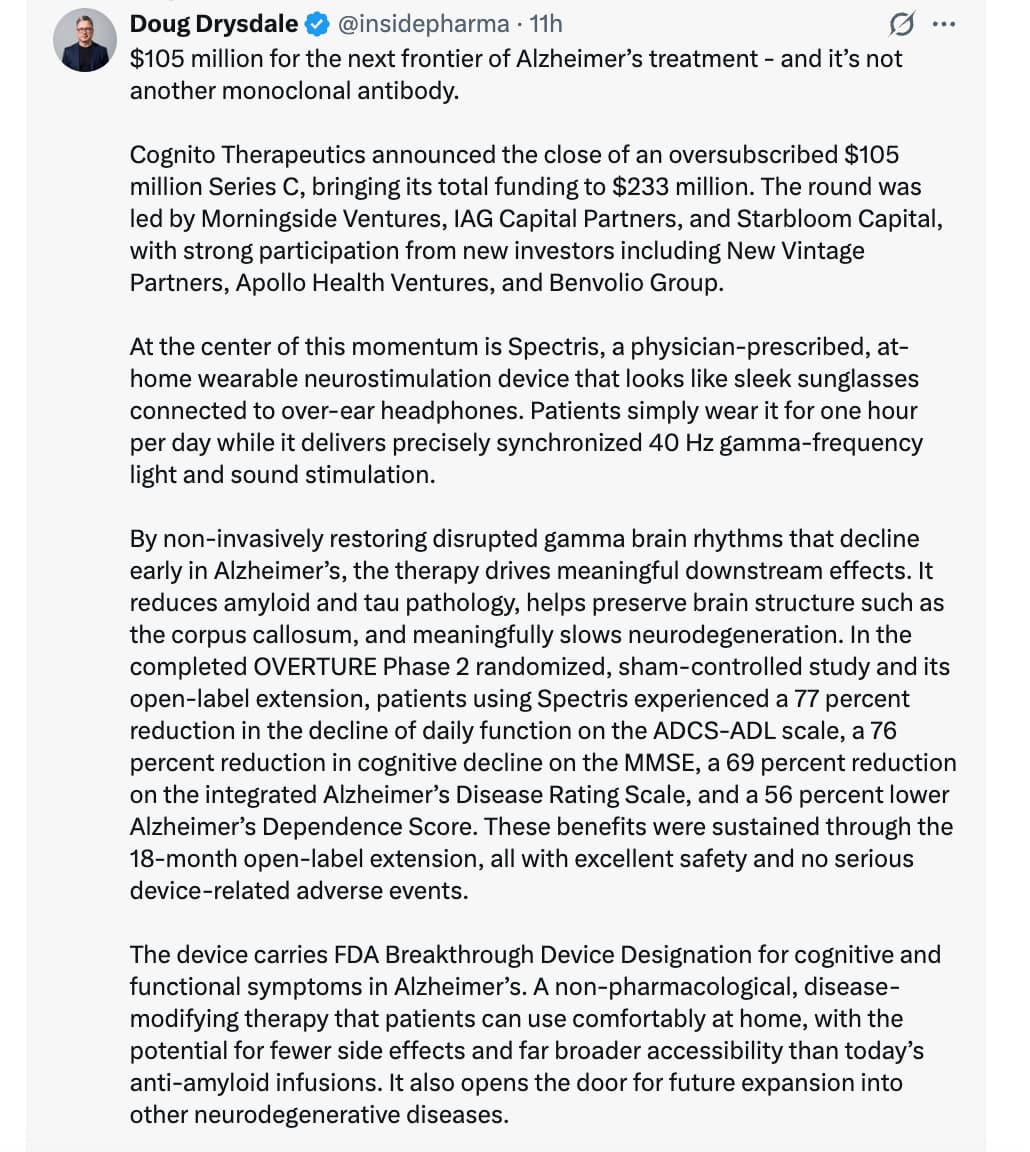
Financing positions company for
pivotal study data readout
FDA submission, and
2027 commercialization in Alzheimer’s disease
And broaden the scientific study and clinical trials to other areas also
while supporting continued clinical development of Spectris™… into additional neurodegenerative indications through their network of brain health collaboratories beginning with WVU Rockefeller Neuroscience Institute.
Spectris has the potential to redefine how a broad category of neurodegenerative diseases are treated
Don’t we want investors to fund science and clinical trials in promising areas when it comes to aging related diseases?
How are we going to know what protocols to adopt, when in life to adopt, etc without scientific studies and clinical data?
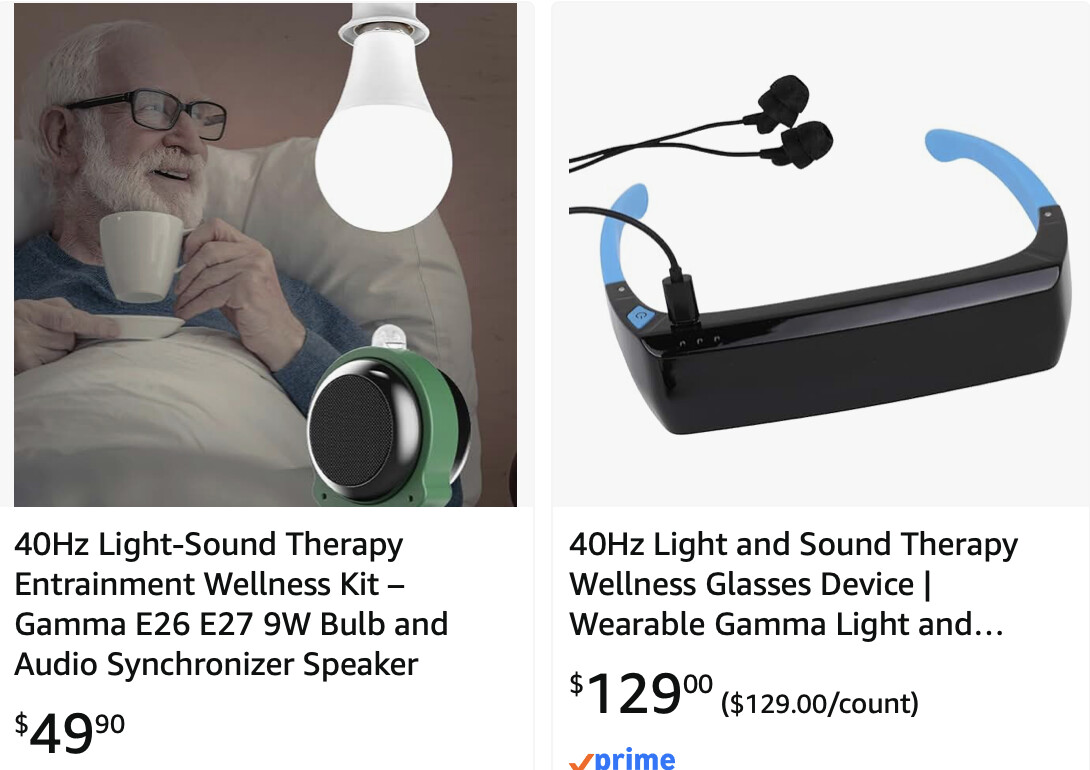
No, what they are trying to do is try to piggyback off of MIT and some other studies. If it were literature, we would call it plagiarism.
The tech to replicate or do new protocols in this area is amazingly simple. It’s IMO just another new bunch of guys trying to get rich. Their endeavors, from what I read on their website, are as high-tech as combining glycine and NAC in one pill, calling it GlyNac, patenting it, and making an easy buck off of fools. Amazingly, they managed to license it to Nestle. Shades of Resveratrol.
And my understanding is that MIT entered a license with the company so MIT has market based upside on any success of the company.
This seems like how we want the system to work.
Top academic scientists can do fundamental, groundbreaking research and the university then benefits from IP licensing. Investors and entrepreneurs can come in and fund and build on what the university originally invented.
And the company can fund continued translational science and large placebo controlled clinical trials to move from mice into humans with different diseases and then enable the approach to get through the FDA.
Even universities like MIT are generally not able to fund large scale clinical work like the company and its investors have in this case.
We need do separate the VC funding issue from the science issue.
The science is legit snd looks promising. More studies are needed and are coming.
On the VC front, they invested $233M which is just insane as they have no real way to protect that.
I looked at their patents applications and most of them have been rejected or are still pending which shows that protecting that is indeed very difficult. I’ve never seen as many patents rejections.
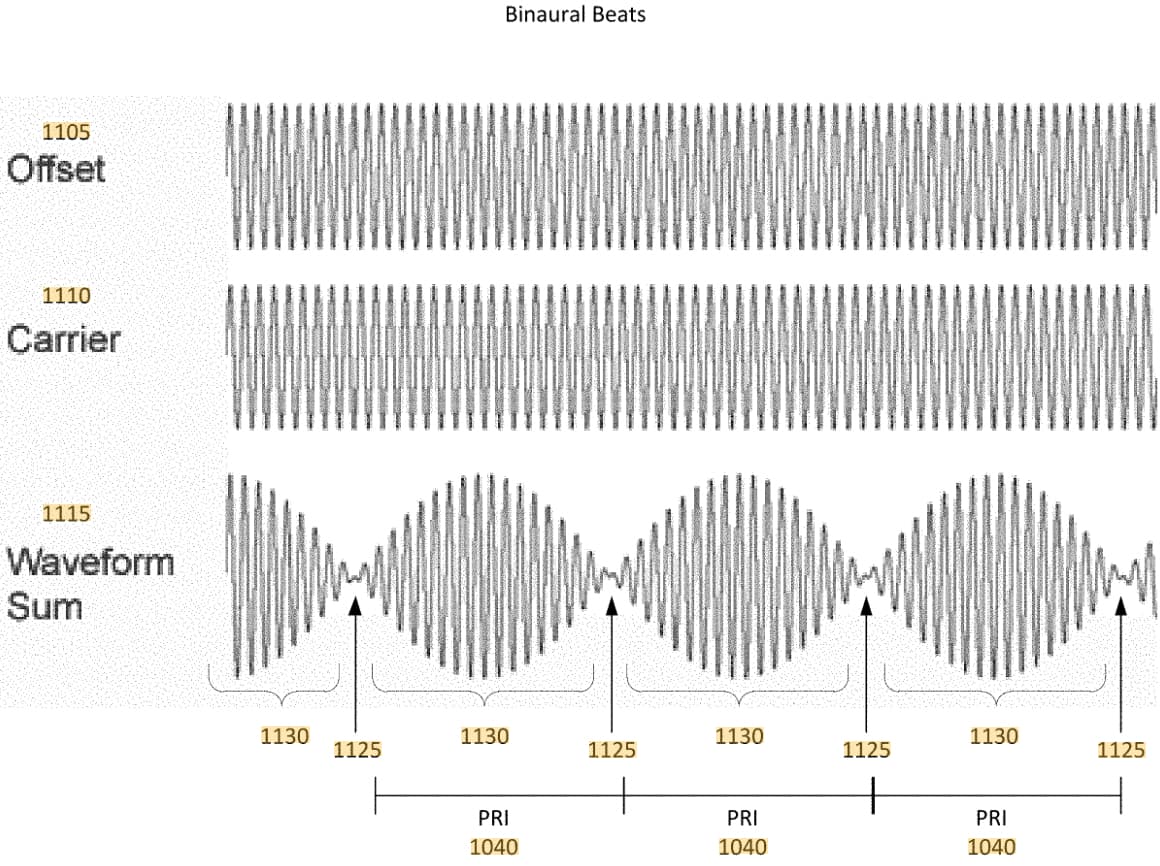
Here is one of them from 2022: Methods and systems for slowing brain atrophy
In that rejected patent they try to describe the use of binaural beats:
Even if they come up with more sophisticated waveforms, those will end up on YouTube as well. You can also use an audio generator app on your phone for generating whatever sound you want.
I don’t know the value of this but the alternative/parallel to a patent is FDA approval. Then they can sell it as a FDA approved device which I assume can’t be used by a copycat.
At some point, it is the only one that can advertise the claim. Now I don’t know if the lack of a patent limits that. Maybe it does. But easy enough to make something secretive about the waveform I would think for the study.
The profit motive is the only thing that will fund the trials. A terrible system but it is what it is. Ideally government could do it but that isn’t the trend we are going towards.
Sorry, I didn’t note that. But it still smacks of BS to me.
This is almost exactly what Dr. David Sinclair did. He also reclassified NMN as a drug to profit from a supplement that was already on the market. The MIT boys have made significant findings in the use of various forms of brain entrainment, but their attempt to profit from low-tech devices by pretending that the devices they use are “special” is just an attempt to profit from their standing as MIT researchers. I don’t begrudge some academics profiting from their studies. But promoting the devices rather than the protocol, to me, is no different than the attitude David Sinclair has.
I don’t think that an FDA approval gives any IP protection. For instance there are plenty of FDA approved BP monitors.
As it’s sound and light it’s pretty easy to record the waveforms. For the sound any phone can record a sound waveform. For light you need something to measure it but it’s very simple and low cost.
Still not following your different posts - do you not want universities, startups and investors to fund scientific research and clinical trials on solutions for aging related disease?
Do you not things in this context now that larger clinical trials have help better calibrate how this technology works in the context of AD and how it does not work there? And what future indication to further clinical trials might be worthwhile while in which other area if may be less worthwhile?
Does it not matter to you to have a better sense of the safety profile of routine usage?
But would a copycat be able to advertise that they were FDA approved? There would probably still be bragging rights of being the original and maybe that is worth $200 million? I mean these people aren’t stupid about money.
I am amazed the money dumping money into medical products and practices and it seems to me not worth it but what do I know?
$200+M seems like a lot of money to do a study to confirm something and it doesn’t seem to have a ROI…I don’t think anyone minds money being spent on research but could be better directed.
How fast are you really aging, and what could that mean for brain health? Aladdin H. Shadyab, Ph.D., explores the gap between chronological age and biological age, and why that difference matters for long-term health. Shadyab describes tools that use information from blood to estimate how quickly the body is aging, including approaches that look beyond the body as a whole to consider aging in specific systems. He connects faster biological aging with higher risk for age-related disease and declines in physical and cognitive function, and discusses how blood-based biomarkers may offer earlier signals of processes linked to Alzheimer’s disease. Shadyab also highlights lifestyle and treatment findings that may support healthier aging and longer survival
Slowing the Clock: Longevity Science Meets Alzheimer’s Prevention
I. Executive Summary
Biological aging, quantified via organ-specific epigenetic and proteomic clocks, diverges significantly from chronological age and serves as a primary, modifiable driver of neurodegeneration and all-cause mortality. Recent analyses utilizing the 30-year Women’s Health Initiative (WHI) dataset reveal that accelerated aging in specific organ systems—predominantly the heart, blood, and kidneys—strongly correlates with the progression of Alzheimer’s disease (AD) and reduced probabilities of exceptional longevity (survival to age 90).
Advancements in high-sensitivity fluid biomarkers, notably plasma p-tau217, extend beyond clinical AD diagnosis. Elevated p-tau217 levels predict incident mild cognitive impairment (MCI) and dementia up to 25 years pre-symptomatically (143% elevated risk) while concurrently serving as a broad biomarker for inverse longevity (30% reduced odds of survival to age 90). Multimarker predictive models integrating 11,000-protein SomaScan arrays, chronological age, and fluid biomarkers improve 10-year dementia prognostication accuracy to a C-index of 0.84.
Therapeutically, the randomized controlled EXERT trial demonstrated that physical activity interventions (120–150 minutes/week) in older adults with MCI, irrespective of intensity (aerobic vs. light-intensity stretching/balance), arrested cognitive decline relative to a usual-care control group. Pharmacologically, retrospective data underscores metformin’s utility; diabetic WHI participants utilizing metformin exhibited a 30% reduction in pre-90 mortality compared to sulfonylurea cohorts. However, robust clinical data for geroprotective pharmacological agents in normoglycemic populations remains insufficient. Interventions targeting foundational metabolic and vascular health, including rigorous adherence to physical activity guidelines and cardiovascular risk mitigation, stand as the most clinically validated mechanisms for decelerating biological aging and extending healthspan.
II. Insight Bullets
Epigenetic Organ Clocks: Accelerated blood, heart, and metabolic epigenetic clocks in women ages 65–79 correlate with a 9–12% increased risk of incident MCI and dementia over 25 years.
Plasma p-tau217 as a Prediagnostic Marker: Baseline elevations in cognitively healthy older adults predict a 143% elevated risk of MCI/dementia up to 2.5 decades later.
p-tau217 as a Longevity Inverse-Biomarker: High baseline p-tau217 levels indicate a 30% reduced odds of survival to age 90, independent of dementia-specific mortality.
Neurofilament Light (NfL) and Lifespan: Elevated NfL, a general fluid marker of neurodegeneration, correlates with a 25% decreased probability of living to age 90.
Inhibition of Healthy Aging: Elevated p-tau217 reduces the probability of reaching age 90 without cognitive impairment by 42%.
Cardiovascular Drivers of AD Biomarkers: Diabetes, long sleep (>8 hours), hypertension, obesity, and smoking actively drive longitudinal increases in plasma AD biomarkers.
Alcohol’s Divergent Impact: Self-reported past alcohol consumption showed a potentially protective effect against the rapid increase of Glial Fibrillary Acidic Protein (GFAP), a neuroinflammation marker.
High-Dimensional Proteomics (SomaScan): Combining 11,000-protein arrays with chronological age and AD plasma biomarkers optimizes 10-year dementia risk prediction models to a highly accurate C-index of 0.84.
Proteomic Organ Clocks: Accelerated protein-based biological aging of the heart, kidney, brain, and immune system directly correlates with increased MCI and dementia incidence (e.g., an “older” heart clock increases MCI risk by 14%).
Kidney Aging Limits Healthspan: Accelerated biological aging in the kidney reduces the chance of achieving healthy aging (survival to 90 without dementia) by 30%.
EXERT Trial Outcomes: Both aerobic exercise and light-intensity activity (stretching/balance/range of motion) over 12 months completely prevented cognitive decline in older adults diagnosed with MCI.
The Danger of “Usual Care”: MCI patients assigned to zero-intervention usual care experienced notable and rapid cognitive decline over 12 months, establishing movement as an absolute biological necessity.
Exercise Volume Threshold: The therapeutic threshold for cognitive preservation in MCI cohorts is strictly defined as 120–150 minutes of weekly supervised or unsupervised movement.
Metformin’s Retrospective Longevity Benefit: Type 2 diabetic women on metformin exhibited a 30% lower risk of death prior to age 90 compared to those taking sulfonylureas.
Metformin’s Translational Gap: Clinical efficacy for slowing biological aging or extending lifespan in non-diabetic human cohorts remains unproven; aging is not an FDA-recognized indication.
Sleep Duration Risk: Sleeping consistently in excess of 8 hours per night serves as an active risk factor correlating with elevated cardiovascular and neurodegenerative biomarker profiles.
Hormone Replacement Therapy (HRT) Risks: The WHIMS trial indicated that estrogen plus progestin therapy in postmenopausal women (65+) actively increases the risk of MCI and dementia.
Structured Physical Activity for MCI: Engage in 120–150 minutes per week of targeted movement. Intensity is secondary to consistency; both aerobic activity and light-intensity stretching/balance regimens halt cognitive decline in early-stage cognitive impairment. Feldman et al., 2022 (Source unverified in live search.)
Cardiovascular Risk Mitigation: Aggressive clinical management of hypertension, diabetes, and obesity to blunt the upward trajectory of neurodegenerative biomarkers (p-tau217, NfL, GFAP).
Sleep Regulation: Restrict sleep duration to the optimal 7–8 hour window. Avoid habitual sleep exceeding 8 hours to mitigate cardiovascular and metabolic deterioration.
Experimental Tier (Level C/D Evidence - High Safety Margins)
Metformin (Normoglycemic Longevity): Retrospective epidemiological data strongly suggests longevity benefits (30% mortality reduction vs. sulfonylureas), but this remains off-label and experimentally unverified in healthy, non-diabetic adults pending the TAME trial. Shadyab et al., 2023 (Source unverified in live search.)
Caloric Restriction: Demonstrates biological age deceleration via epigenetic clocks in clinical settings, though long-term compliance and risks of sarcopenia/frailty in advanced age cohorts demand strict clinical supervision. Belsky et al., 2023 (Source unverified in live search.)
Red Flag Zone (Debunked or Safety Data Absent)
Asymptomatic p-tau217 Screening: FDA approval is strictly limited to symptomatic individuals for AD diagnosis. Routine screening in cognitively intact adults is biologically un-actionable, lacks preventative protocols, and carries high psychosocial risk.
HRT for Late-Stage Dementia Prevention: Prescribing estrogen plus progestin for the explicit purpose of dementia prevention in late postmenopausal women (65+) is actively contraindicated by WHIMS trial data. Shumaker et al., 2003 (Source unverified in live search.)
Direct-to-Consumer Epigenetic Aging Clocks: Commercially available biological age tests currently lack standardization, regulatory oversight, and clear clinical intervention pathways.
Exercise can lower Alzheimer’s risk. Scientists may have discovered why. (WaPo)
In an ambitious study, memory and learning abilities improved substantially after exercise among mice with a form of Alzheimer’s disease.
Exercise can strengthen a leaky blood-brain barrier, which may improve brain health and potentially fight dementia, according to an ambitious new mouse study of exercise and neurodegeneration published this month in Cell.
In rodents and people, the blood-brain barrier — a narrow layer of cells that protects the brain from toxins and pathogens — typically weakens with age, contributing to neuro-inflammation and other problems, including heightened risks for dementia. But the study’s authors found that during and after exercise, at least in mice, the liver releases a specialized protein that travels to the brain and helps repair the protective cellular barrier there.
The effects of the exercise protein were especially striking in older mice with a form of Alzheimer’s disease. Their memory and learning abilities improved substantially when levels of the protein rose in their brains.
The researchers found the same protein in the bloodstreams of physically active people.
“These results provide compelling evidence in animal models that exercise-related signals from the liver can improve brain function by acting on the blood-brain barrier,” said Michelle Voss, a professor and director of the Health, Brain and Cognition Lab at the University of Iowa. She studies physical activity and the brain but wasn’t involved in the new study.