Yes it’s frustrating how slow trial results come out. You can often get them faster by contacting the authors. For instance the results of this trial are not yet out ( Risk Reduction for Alzheimer's Disease - Full Text View - ClinicalTrials.gov ) but the author told me that it failed: 2y of intensive BP control with losartan and amlodipine + physical exercise did not improve cognitive performance.
Yes I’m aware of the hypotension risk in PD but I’d still look at BP, especially continuously over a day or week (for instance with a device like Aktiia) because:
- Hypertension in mid-life may be a risk factor for PD later in life: Hypertension and Diagnosis of Parkinson’s Disease: A Meta-Analysis of Cohort Studies - PMC
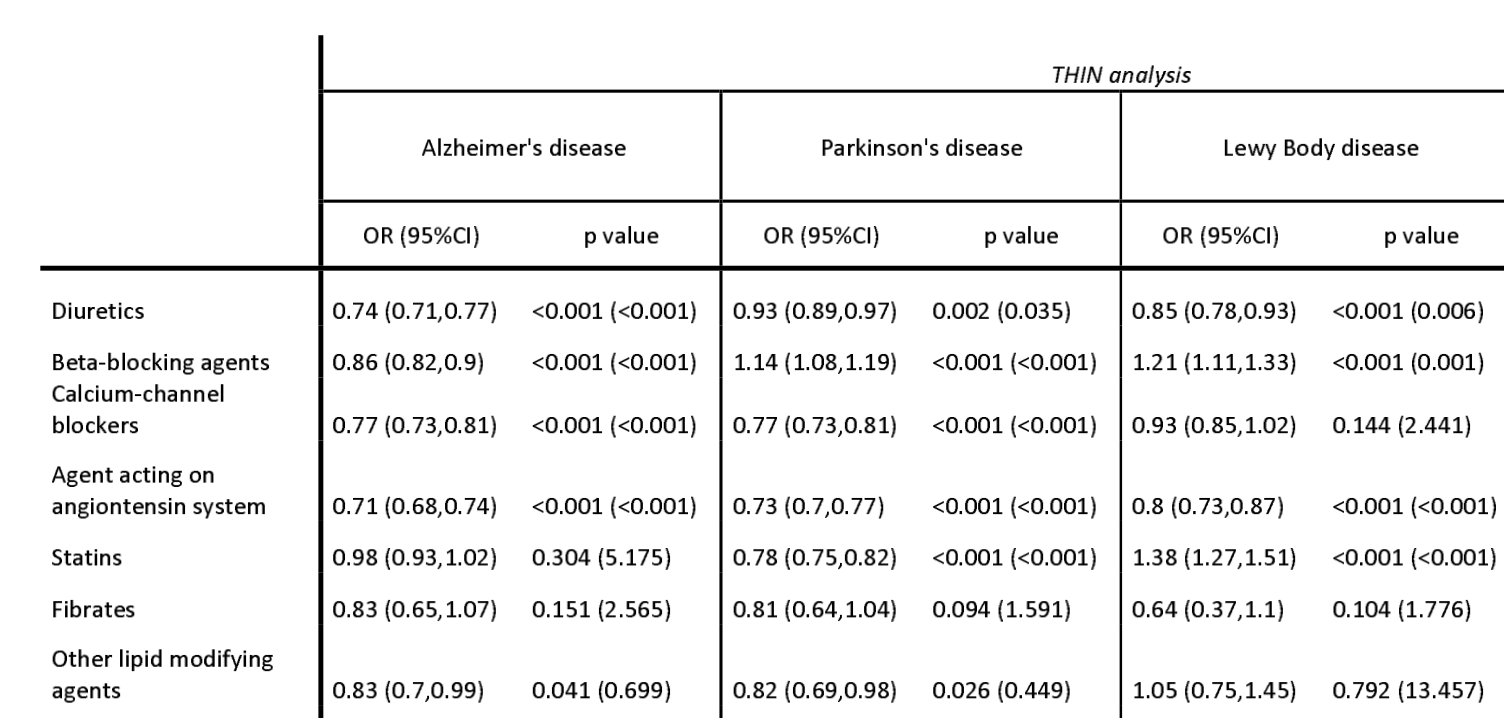
- Some antihypertensive drugs are considered as potential repurposed treatments for PD (namely CCBs like isradipine and ARBs like candesartan/telmisartan)
- Blood pressure variability (BPV, aka the variations during the day and week) seem to matter more than the mean for neurological diseases. Maybe you spend a lot of time during the day in hypotension and/or hypertension and don’t know it. And it seems that CBBs and ARBs can “smooth” the BP (without reducing it too much at low doses). See: Blood pressure variability: methodological aspects, clinical relevance and practical indications for management - a European Society of Hypertension position paper 2023
- Knowledge is power.
- It may be useful to detect and manage orthostatic hypotension: Smartwatch May Help Parkinson’s Patients Manage Blood Pressure Drops
Regarding telmisartan/candesartan, see as well: The Endotoxin Hypothesis of Parkinson’s Disease 2023:
If LPS contributes to PD, then a number of possible therapeutic strategies could be considered for further evaluation in clinical trials as outlined below. However, if LPS is elevated in only a subset of PD, patient stratification would be essential for targeting the most appropriate patients. Monitoring of blood LPS levels in such trials would provide important validation of the mechanistic principle, alongside clinical efficacy measures. […] (4) Blocking LPS receptors. Candesartan, an existing drug licensed for the treatment of hypertension, has been shown to reduce TLR4 expression and activity, is expected to cross the BBB, and has a good safety profile, making it an attractive candidate for repurposing in Parkinson’s disease.
Does anyone know how to test for serum LPS?
I’m also curious:
- Are there things that you tried but stopped because they did not seem to work or had bad side effects?
- Among all your interventions, if you had to keep only one, which one would it be?
- Have you considered selegiline/deprenyl at a low dose? (it may protect the BBB from LPS, see: Anyone taking Selegiline / Deprenyl For Longevity? - #55 by Vulcan )