Thanks for a good share - have you - or anyone else - seen anyway to test our levels?
The article cites this paper: Urolithins: potential biomarkers of gut dysbiosis and disease stage in Parkinson’s patients 2022
There they say:
Urolithin detection in urine is a feasible, non-invasive and fast approach that can reflect gut microbiome dysbiosis and intestinal inflammation in Parkinson’s disease patients.
Stool samples were collected for the gut microbiota analysis at baseline, while urine samples were collected for the urolithin analysis after consuming 30 g of walnuts for three days, a short polyphenol-rich intervention in which participants can produce urolithins. Urolithins were determined in urine samples by ultra performance liquid chromatography–electro spray ionization–quadrupole time of flight–mass spectrometry (UPLC-ESI-qToF-MS) as previously described.
They cite:
Ellagitannins and ellagic acid (EA) are metabolized by the gut microbiota to produce urolithins that could be responsible for the health effects attributed to ellagitannin-containing food products. Several urolithin aglycones could be present in fecal samples while glucuronide and sulphate conjugates are mainly found in plasma and urine. So far, the lack of available standards has made difficult their correct identification and quantification. In the present study, UV and MS spectra characteristics of urolithins and their phase II metabolites have been determined using different systems based on liquid chromatography (LC) coupled with diode-array or mass spectrometer detectors with different analyzers (triple quadrupole (QqQ) and quadrupole time-of-flight (QTOF)). Chromatographic separation was achieved on a reversed-phase Poroshell C18 column (3×100mm, 2.7μm). Elution order, characteristic UV spectra, and relative response factors (RRFs) with respect to their parental compound (EA) and the most common metabolite urolithin A (Uro-A) were determined. This contribution, along with the most important mass spectra characteristics (MRM transitions, qualifier/quantifier ratio, accurate mass and fragmentation pattern) will allow the determination of urolithin metabolites in different biological samples and their quantification even if not all metabolites are commercially available. The methods developed in the three systems have been fully validated in terms of linearity, sensitivity, precision, recovery, matrix effect, selectivity and stability. After that, they were successfully applied to complex biological matrices (urine, feces and plasma) from two human studies in which volunteers consumed ellagitannin-containing foods, such as walnuts and pomegranate extracts.
So you need UPLC-ESI-QTOF-MS. How much does this cost? Or can you access it from a lab?
[Update: OK 10 to 100k$: Waters SYNAPT G2 ]
1 Like
Seems like something that one of the current testing companies, perhaps Jinfinity, Genova Diagnostics or Iollo could offer.
There was another source I think you or something else shared the last day or two where one could just do it from a blood spot card.
Wonder what Mitopure did for their different clinical tests. @RapAdmin did they even offer to test people’s levels in the past or something - I think I recall something like that from some post you made, but perhaps it was something else than Mitopure/UA?
1 Like
I’d be ready to pay to rent a UPLC-ESI-QTOF-MS from a lab and test my sample…
1 Like
I think they offered a free test to see if your gut microbiome could produce urolithin A from pomegranate juice.
https://www.timelinenutrition.com/blog/making-a-natural-anti-aging-nutrient-available-to-everyone
1 Like
Yes - I still have the kit in the bedroom… did the test, but never mailed it in because I got busy with other things. See here: Urolithin A - Virtual Clinical Trial by Timeline Nutrition
I remember a podcast with one of the guys at the Buck Institute and apparently its a pretty easy, quick and inexpensive test (In the Timeline trial, you just dripped a few drops of blood on a piece of paper and sent it to them). Someone needs to create a commercial version of this test - perhaps if a bunch of us emailed a few test labs like Merek, and Life Extension foundation, they would offer it.
2 Likes
Interesting paper confirming the view of PD as a disease of aging: Dopaminergic neuron loss in mice due to increased levels of wild-type human α-Synuclein only takes place under conditions of accelerated aging 2024
1 Like
It will be interesting to see what diseases are affected by hitting the key aging pathways.
1 Like
Cholesterol, dementia, and PD (Cont’d): Differential effects of cholesterol levels on cognition according to body mass index in Parkinson’s disease 2024
lower TC levels were associated with lower composite scores of frontal/executive function and a higher future risk of PDD conversion in the under-/normal weight group, whereas higher TC levels were associated with poor performance on frontal/executive items and more frequent PDD conversion in the obese group. These findings indicate that the association between TC levels and cognition is moderated by BMI in patients with PD, suggesting that a cholesterol-lowering strategy could be applied differentially according to BMI.
Clinical studies have demonstrated that individuals with high levels of circulating TC are less likely to develop PD and have better long-term outcomes.
A recent investigation discovered that elevated cholesterol levels have a dual role in PD: they protect against lysosomal membrane permeabilization while also promoting α-synuclein accumulation
When examining the association between cholesterol levels and Alzheimer’s disease or vascular dementia, previous studies have shown inconsistent results, and this association seems to vary with age at measurement (mid-life [< 65 years] or later life [≥ 65 years]) and follow-up duration
Causal relationships could not be assessed in this study, and reverse causation should also be considered. For example, because TC levels are biomarkers of malnutrition, patients with PD who have low TC levels in the under-/normal weight group may be malnourished, which subsequently leads to poor cognitive outcome. In addition, a recent study showed that familiar patients with PD, particularly those with a glucocerebrosidase (GBA) mutation, have lower cholesterol levels than healthy controls and patients with sporadic PD. Considering the fact that GBA is associated with poor cognitive performance and the risk of PDD, poor cognitive outcomes in patients with PD and low TC levels in the under-/normal weight group may be attributed to underlying genetic risk factors.
1 Like
In vitro modulation of mTOR and mGlur5 influence α-synuclein accumulation 2024
We found that both rapamycin and CTEP induced a significant reduction of α-syn fibrils in SH-SY5Y cells and this effect was associated with a reduction in mTOR signaling and enhancement in autophagic pathway factors. These data support the possibility that CTEP (or rapamycin) might be a useful pharmacological approach to target abnormal α-syn accumulation by promoting intracellular degradation or enhanced clearance.
And another paper about another immunosuppressant, tocilizumab: Researchers identify immunomodulatory drug as a potential treatment for Parkinson’s disease
1 Like
Recent articles of various quality but pointing to the same direction: telmisartan seems good for PD.
- Angiotensin type 1 receptor activation promotes neuronal and glial alpha-synuclein aggregation and transmission 2024
- Investigating the neuroprotective effects of Telmisartan using the lipopolysaccharide rat model of Parkinson’s disease 2024
- Telmisartan Protects Mitochondrial Function, Gait, and Neuronal Apoptosis by Activating the Akt/GSK3β/PGC1α Pathway in an MPTP-Induced Mouse Model of Parkinson’s Disease 2024
Expect clinical trials of telmisartan in PD soon…
I am interested in any papers or animal trials related to Parkinson’s or even any anecdotal evidence of benefit of Rapamycin in Parkinson’s.
4 Likes
It seems like it may provide some benefit. I recommend you hunt around on Pubmed…
There appears to be some linkage between age-related essential tremors and Parkinson’s disease.
FWIW:
Before I started rapamycin, I am 82 years old, I was experiencing age-related essential tremors. After a few months of rapamycin, they completely disappeared. This was something I was not expecting and did not notice it until it occurred to me that my hands were not shaking when eating.
This study was of course on mice, but it certainly gives some hope.
“Rapamycin can effectively alleviate symptoms of PD”
4 Likes
Thanks for this - very interesting. What dose of rapamycin are you taking? As far as PD goes, I am interested for a patient of mine with very early symptoms. I’ve had a mild essential tremor for years and have been on the rapa for less than 3 months ago I’m looking forward to seeing if any of those things change.
5 Likes
I was following a suggested protocol at the time based on Dr. Mikhail V. Blagosklonny’s work and Twitter feeds.
So like most here, I am self-experimenting. I started off with 5mg/week with EVOO then tried 20mg with GFJ and EVOO once every two weeks.
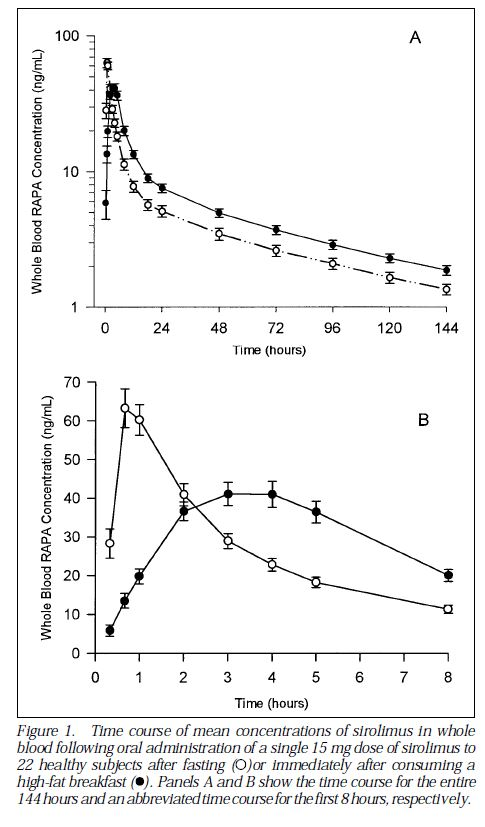
Blagosklonny’s recommendation at the time was pulse dosing at the maximum amount that did not produce unwanted side effects. The 2-week pulse regimen is based on allowing 5 half-lives to occur between doses. The current popular 1-week regimen is apparently based on mTOR modulation. The 20mg with GFJ and EVOO may have been equivalent to ~40 to 80 mg of rapamycin. Some will think this is a foolishly high dose, but it has been pointed out that even massive overdoses produced no lasting adverse effects.
The 20mg with GFJ produced mild diarrhea on the second and third days after taking the dose.
I now am titrating back up to the max I can take with GFJ. Right now I am taking 5mg/week with GFJ and EVOO. This dose produces no apparent side effects. I get blood work regularly and try to keep my lipids in the “normal” range.
I am 82 and a self-experimenter and do not recommend to anyone to follow anything I do.
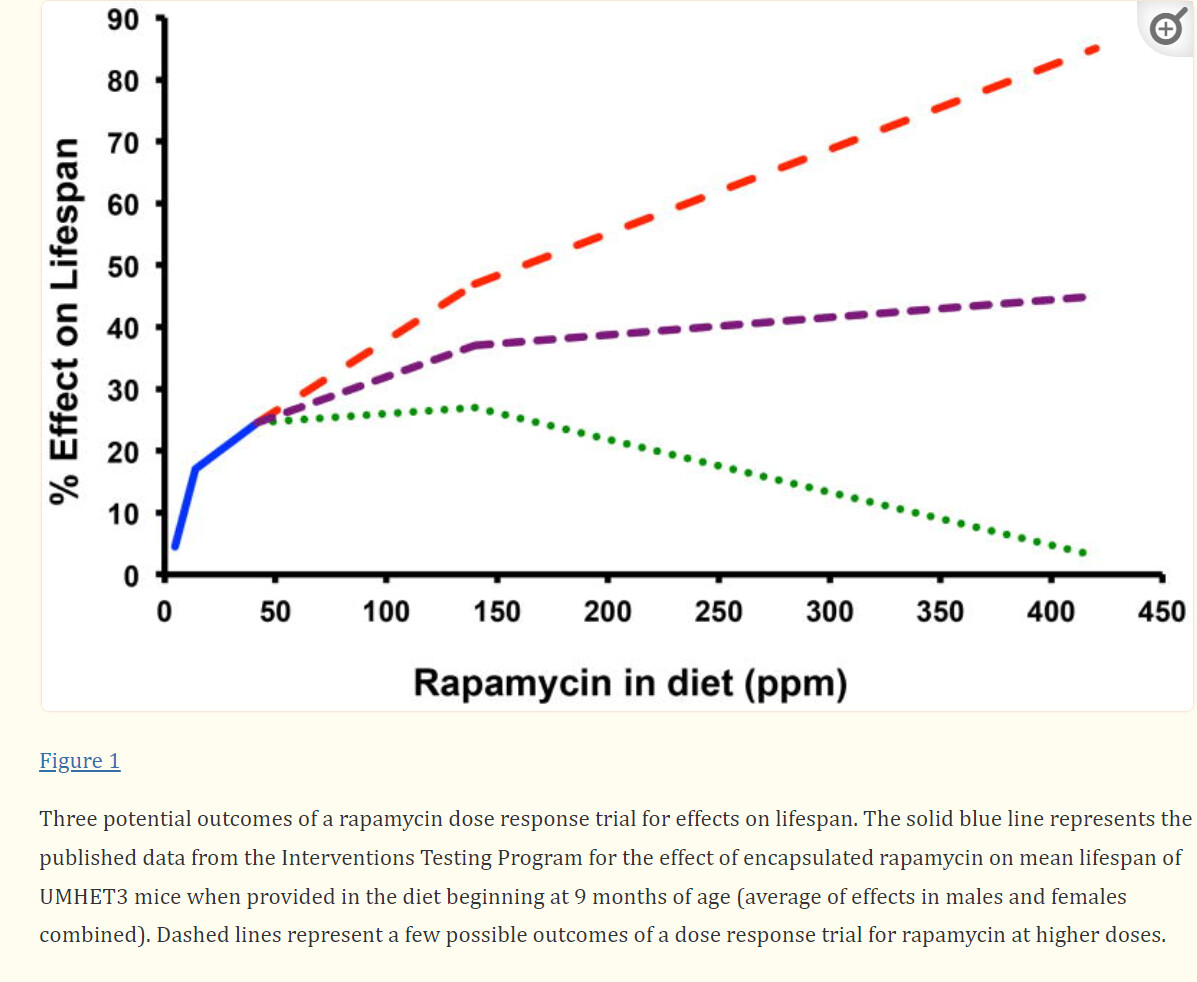
Most studies for longevity indicate higher doses for longer lifespans.
These charts have been posted before, but I will save you the trouble of looking for them.
4 Likes
There doesn’t seem to be much in the way of online evidence, does there? But I have PD and I’m trying it–8mg/week since December. Had PD for 8 years…can’t say I see much difference yet and wonder if I should dial it up. But I also fast and eat keto, so maybe that’s confounding?
1 Like
I think the effects are likely to be slower than that. In terms of dialling it up, have you had any side effects at 8mg? It probably depends on your age and weight as well. Are you taking meds for the PD?
1 Like
Ha, yes, I guess I know that. Really, the best I hope for is a slowing or (dare I say) stopping of progression, and of course, that’s nearly impossible to measure.
No side effects yet (keep waiting for pimples!) and I wonder about dialing it up but I’m a little scared. I’m 66 (as of yesterday, actually! :o) and pretty tall + skinny. 140lbs.
My symptoms are still one-sided. I don’t take any dopamine. I take rasagiline because when I was diagnosed there was a study that suggested a hint of neuroprotection and my Dr. was all over it. Not sure it does much.
I take a stack of supplements–the usual, probably, for this crowd. What I believe (with no hard evidence) has helped the most is exercise and DIET–as I said I eat keto, and fast. And oh yes, I have a GBA mutation…if that means anything to you.
2 Likes
I have Parkinson’s since December 2020. I do not take any medication! Since three weeks I take 5 mg rapamycin a week. I have published a video about my alternative healing methods:
")
8 Likes