A new paper that ranks the top anti-aging drugs, with a slightly different ranking and rating system that I’ve seen before. But no new therapeutics here - just a slight reranking of all the usual suspects.
Of course, animal studies of the combinations of all these different drugs are long overdue. Many people are already combining these drugs in their own personal anti-aging cocktail, but we really don’t know the combined effects of the drugs.
Discussion:
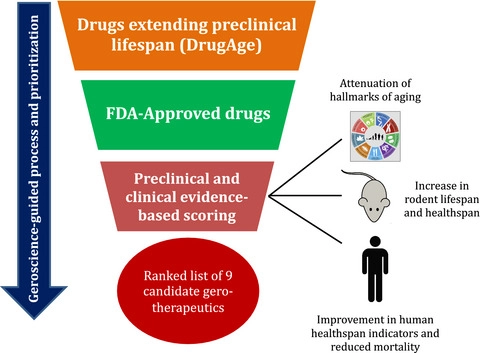
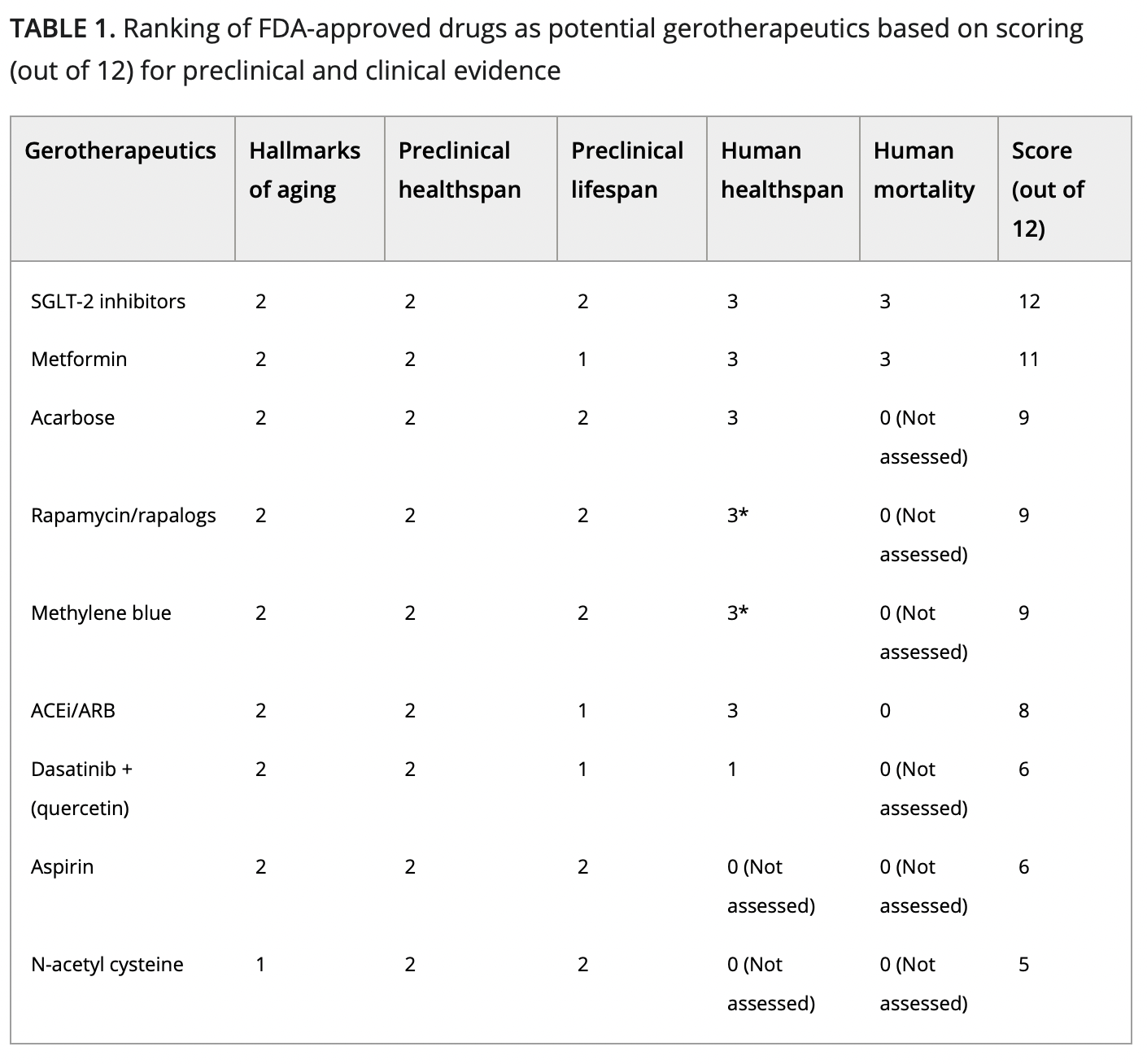
We provide a rigorous assessment of the literature concerning both preclinical and clinical status for several FDA-approved potential gerotherapeutics. We developed a scoring scale that equally values (6 points each) the preclinical and clinical evidence supporting the claims for each of the nine potential gerotherapeutics selected. Surprisingly, with a score of 12/12, the best evidence was found for a relatively new class of drugs, the SGLT2i, which showed better promise than other known potential gerotherapeutics such as metformin, rapamycin, or acarbose.
The profound effects of SGLT2i on healthspan and lifespan in both animal models and humans may result from the pleiotropic effects beyond renal glucose and sodium handling, including improved mitochondrial function, restoration of autophagy, and promotion of ketogenesis-dependent dampening of mTORC1 hyperactivation (Durak et al., 2018; Korbut et al., 2020; Tomita et al., 2020). We also identify several drugs that, like metformin, are relatively low-cost molecular entities with a well-established safety profile, representing possible candidates for inclusion in a geroscience-guided clinical trial modeled after TAME, and aimed at probing whether a predefined cluster of age-related diseases or well-characterized loss of function can be significantly delayed using an approach based on targeting aging biology. Moreover, our geroscience-guided literature-driven approach is concordant with previously proposed data-driven drug repurposing approaches using evidence from gene expression or model organism studies, with the overlap of rapamycin and senolytics identified as top candidate drugs across these (Dönertaş et al., 2018; Ziehm et al., 2017).
For our analysis, we decided to assign an equal number of points to knowledge derived from geroscience (i.e., preclinical) and to findings from humans (i.e., clinical—both observational and interventional). Although for translational purposes, knowledge from human studies is likely to have more weight than studies in rodents, we gave both equal values for several reasons: (1) The literature on potential gerotherapeutics in rodents is quite extensive and, while many of these studies are too recent to have been considered for clinical trials yet, their potential should not be dismissed based solely on their “novelty”; (2) some mouse studies, like the ITP, are quite robust, thus enhancing their predictive value as potential gerotherapeutics; (3) because of their highly controlled nature, studies in mice often have fewer caveats than similar studies in humans. Thus, while it could be argued that preclinical geroscience knowledge becomes less relevant if a drug has solid data on decreasing all-cause mortality in humans, we decided it was not appropriate at this time to penalize potential drugs that have strong preclinical evidence.
Full paper here:
Geroscience-guided repurposing of FDA-approved drugs to target aging: A proposed process and prioritization
An Updated Prioritization of Geroscience- Guided FDA-Approved Drugs Repurposed to Target Aging
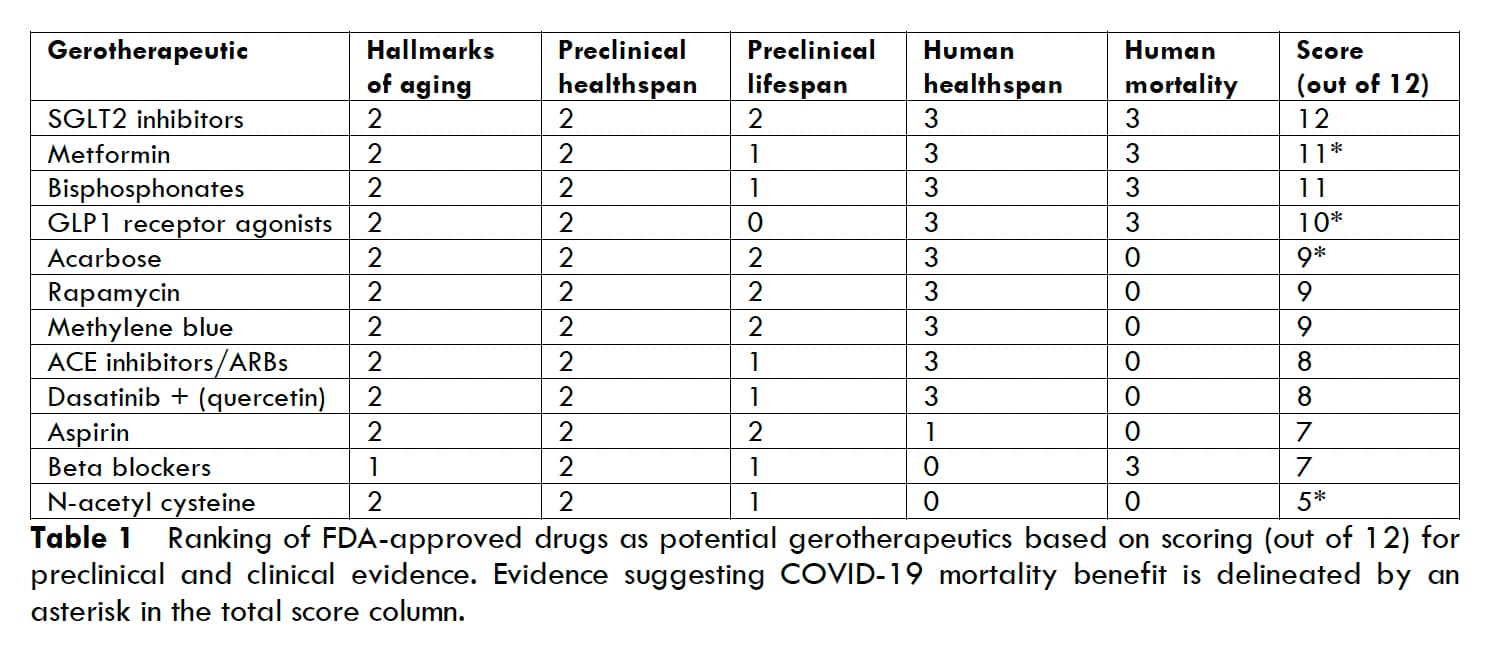
The biological mechanisms of aging drive the development of chronic diseases such as cardiovascular disease, diabetes, dementia, and cancer that dominate our current medical system. Geroscience-guided approaches seek to mitigate these pathological consequences of aging by targeting the fundamental hallmarks of aging. Using modalities that modulate these aging mechanisms to reinforce longevity we can prevent the onset of these diseases as well as target many of them at once. In this way, geroscience-guided approaches hope to extend both lifespan and healthspan in the near future. This article builds upon a previous paper which proposed a standardized process for evaluating FDA-approved medications for their geroscience potential and prioritized them to reflect preclinical and clinical evidence. In this article, we provide an update of the previous list of candidate gerotherapeutics to reflect the new and rapidly evolving evidence. We include the geroscience-guided evidence for three new FDA-approved drugs which did not have strong arguments for inclusion before: bisphosphonates, GLP-1 receptor agonists, beta blockers. This updated prioritization should help guide the efforts and financial investments for translating geroscience and allow immediate progress involving such candidate gerotherapeutics, especially the top 4 drugs: SGLT2 inhibitors, metformin, bisphosphonates, and GLP-1 receptor agonists. Since all of these drugs have been approved for safety and used extensively, repurposing them as gerotherapeutics should be considered in older adults.
I haven’t read the paper.
One thing I don’t see them weighting is the risk of side effects.
For example, I thought bisphosphonates carried a risk of bone necrosis (someone please correct me if wrong) which, if it happens, is pretty serious.
@RapAdmin This is one of the most important posts I’ve seen on this board. I agree with @DrT .
Interestingly, I’m taking a high % of those on the list, and advise them to patients. The one that is #1 on the list, SGLT2 inhibitors is not something I take or routinely advise, nor are bisphosphonates, methylene blue, aspirin or beta blockers.
The only reason some items aren’t scoring higher is due to “Not Assessed.” Also the degree of benefit is not clearly characterized.
The specificity also is an issue - for example with ACE and ARB are these agents that cross the blood brain barrier or not - same issue with Beta blockers on the last report.
On the NAC - what about NAC Ethyl Ester … The evidence on aspirin is contrary to what they cite - the evidence is most clearly stated with the USPSTF - in that most people end up with harm rather than benefit with taking this.
So targeting whatever they are looking at here might not actually be the best approach. It is however a fascinating paper and scoring system. It is arbitrary and not indicative of size of effect.
I’ve seen a few serious perineal infections with SGLT-2 inhibitors, but this is in diabetics. We don’t clearly see in this paper, was this in non-diabetics that SGLT-2 inhibitors have this great profile. Given that they result in you passing glucose into your urine – does this benefit someone who doesn’t have diabetes?
+1. Putting “ACE/ARB” as one category is weird. (I think half life is more important than BBB crossing btw.)
Yes. They also reduce heart failure, kidney damage, liver damage, arrhythmia, atrial fibrillation, and atrial flutter in non diabetics. And they decrease body weight and blood pressure a bit.
We had a good look at the evidence for metformin on this forum and it appeared that the evidence for its use by non diabetics was not strong. Indeed it appeared to be subject to selection bias.
I have a strong preference for Telmisartan as there are a host of research on this being significantly beneficial for neurocognitive decline. It has a long half life - but lisinopril does also, and crosses the BBB, but doesn’t seem to have the same benefit. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9125564/
I often discuss with patients, that if they have adequate blood pressure - let’s get you on Telmisartan … it seems like a great anti-aging and cognitive protective agent. So many people look at their blood pressure as a negative thing – instead, it is an opportunity to introduce medications that can decrease risk of death and disability.
On the SGLT2 agents, I am going to take a fresh look at these, as there are costs (not so bad if purchased off shore) that can be prohibitive for many patients. I’m biased as I’ve seen some complications, but this is in a select population that have been taking very poor care of their health. That is not the demographic that I’d be considering these agent in, in this context.
Which of these are proven in clinical trials? I think it’s important to differentiate them based on level of evidence. HF and kidney damage I know.
@DrFraser this is a nice article on the history of gliflozins:
After flozins were approved as diabetes drugs, on the basis that they lower the markers of diabetes, they had to go through further trials to be sure that they did not increase the risk of heart attacks, strokes, or deaths due to cardiovascular disease. This requirement was imposed by the FDA in 2008, after a meta-analysis published in 2007 found that rosiglitazone, another diabetes drug approved on the basis of surrogate endpoints, increased the risk of heart attacks by 43 percent.
These trials were imposed to confirm the benefits of the drugs were not outweighed by cardiovascular side effects.
Yet something unexpected happened: the trial for empagliflozin – which, like dapagliflozin and canagliflozin, inhibits SGLT2 much more strongly than SGLT1 – showed a 14 percent reduction in major cardiovascular events, a 35 percent reduction in hospitalizations for heart failure, and a 38 percent reduction in cardiovascular deaths overall – all statistically significant.
@adssx
The issue with most studies on these drugs is the use in pretty unhealthy individuals where we are looking at progression of disease in patients with heart failure or chronic kidney disease, or are at high risk of developing those issues.
Giving these agents to a healthy individual likely has markedly less (or no) benefit, would be my concern. The mouse data is interesting, but I’m not sure how this class of drug gets to the top of the list of longevity medicines. I however will go through the other thread in some detail, as I get my feed of articles from Journal Watch, and they are unlikely to put forward articles using these agent in healthy individuals.
They’re approved for CKD, T2D and HF and in these groups they tend to prevent the other disease. Said otherwise, if you only have T2D and no CKD or HF, SGLT2 will still protect your kidney and heart (and brain also btw). And more than other glucose-lowering drugs. So they already protect people with a healthy kidney or heart (for instance).
The % of the population (at least in the US) with diabetes, pre diabetes, HF, pre HF, kidney disease or “pre CKD” or at high risk of these (because of family history, genes, age, etc.) is so high that most individuals, including “healthy” ones would fall in one of these buckets.
Given the ongoing trials, we can expect SGLT2i indications to be extended to arrhythmia, atrial fibrillation, and the various liver diseases (NAFLD, etc.). This will make the case for SGLT2i even stronger.
Quoting Brad Stanfield: “In terms of a so-called longevity medication, I think that SGLT2 inhibitors will be the first ones that will be prescribed and made widely available. That’s because they appear to provide significant protective effects for the kidneys. Our kidney function starts to decline from around the age of 30, so if we can use SGLT2 inhibitors to slow down or prevent that decline, that would be a powerful intervention. Of course, we’re waiting on the human data to come through, but there is a robust way of these things getting through to people.”
Probably the bigger challenge is whether one gets any additive effect of adding an SGLT2 inhibitor to rapamycin plus metformin plus acarbose? Are we simply hitting the same pathways, and if so, is adding another agent having any benefit.
When treating T2DM, I’ve usually gone with metformin+acarbose and a GLP-1 agonist as first line for glycemic/metabolic control. However, the SGLT2 inhibitors have some other unique benefits.
Working in the ER and seeing complex UTI’s and perineal infections in patients with use of these agents creates some concerns, but none of these were in people who were fit and healthy in any respect.
Anyway, great post, and well worth taking a serious look and think on.
Good question. But as far as I know rapa/metformin/acarbose don’t protect the kidney and liver for instance. The pathways of SGLT2 inhibitors are not known. Here are three other good reviews of SGLT2 inhibitors’ effects btw: Acarbose - Details On Another Top Anti-Aging Drug - #448 by adssx
As you seem to like low-dose combinations, in George Medicines’ pipeline there’s GMRx4, “containing three existing best-in-class drugs and formulated at an ultra-low dose: metformin XR 350mg, dapagliflozin 2.5mg and sitagliptin 17.5mg”.
I have a lot of patients with chronic kidney disease or heading that direction, and certainly going with an SGLT2 makes sense, for those without those factors, and for a healthy individual, it certainly has me looking a bit more at these, and at least adding it to the list.
So many patients have obesity, and I still favor the Glps in those patients as they work on every component of cardio metabolic syndrome. However as sole agents don’t get the glucose down enough.
The GLP’s should be on this list as there are clearly benefits, including longevity - perhaps the data is just lagging on these.
Your input certainly has me putting these as next agents.
Metformin failed at NIA ITP, also after Metformin success with humans, there were 5 previously unpublished papers that showed no benefits even in diabetics
SGLT inhibitors extended lifespan in NIA ITP - but only in male mice, in female mice 0%
Mehylene blue failed NIA ITP
Aspirin extended lifespan at NIA ITP but only in 1 test from 3 (and only in mice)
Rapamycin is the most robust from all of this - but even then effect is not as strong as Rapamycin + Acarbose, and dose in mice is 10x higher than what people take
I think the jury is out on longevity outside of obesity patients
seems very anti one of the main longevity pathways to continuously rev up insulin release into the blood 24/7 vs the normally rythm of it only going up after a meal and only as much needed depending on the type of meal and then going back down to low levels again
cancer risks might not have been to big for a few years of use, but what will that look like after a decade or several decades on them
There is a consistent improvement in metabolic syndrome, which increases essentially every bad health outcome. Reverse this, which these agents effectively do, and a huge percentage of the population suffers from, and we know the impact expected on longevity.
These agents do not consistently increase insulin, except in those with significant high blood sugar - which I’d argue should not be what we are primarily depending on this drug for (it should be in combination with others). They do improve insulin sensitivity, which then leads to less insulin needing to be produced.
There is reasonable literature on likely improvements in risk of neurocognitive disease. We know obesity increases malignancy - I’ve not seen any evidence to support a risk of malignancy, short or the rare cases in MEN patients. But yes, we’ve only had this class of medications, I think since 2005. We’ve seen almost 2/3rd reduction in risk of developing Parkinson’s Disease in one look at patients on a fairly weak GLP-1 agonist.
Overall, I don’t know if for the ideal body weight insulin sensitive individual whether this is helpful, but that isn’t the typical person I deal with.