Thanks for the info man, will try that.
1 Like
Also Clammy, fenofibrate and other fibrates lower uric acid a lot. Mine was 4.3 last time
don’t believe anything about biological age calculation. Those people who think they can make any correlation or usefullness out of that are as full of crap as the day is long. About as reliable as a soothsayer , faith healer , palm reader etc.
1 Like
A small update about what I’m tracking.
I recently bought a Body Cardio Withings scale to track body composition, and more importantly, arterial stiffness via pulse wave velocity (PWV). There are at least 2 small studies that validate the accuracy of this scale when it comes to the gold standard for PWV, here is one of them:
This has proven useful to me so far, and that data along with Garmin (VO2max estimation) has shown me that my curent training is currently lacking, and I either need to start adding more intensity, or more duration. I’ve opted for more intensity because I need to start at serioulsy improving my VO2max anyway.
I’ve also decided to ditch my use of acarbose, and instead add intermittent use of empaziflogin (Jardiance). Part of it is that I’ve been at a weight plateau for the last 6-9 months. The other part is for the potential longevity and cardiac benefits.
There are 2 things that I find interesting with empaziflogin. First, that one study shows that even intermittent use over a long period confers some benefits.
The intake rate of empagliflozin was 96.7 ± 7.2% for the regular group and 45.7 ± 7.0% for the intermittent group. Interestingly, ΔHbA1c was identical in the two groups (-0.64 ± 0.19% and - 0.65 ± 0.17%, respectively). Body weight decreased (-2.72 ± 0.52 and - 1.50 ± 0.45 kg, respectively) and diabetes treatment-related QoL increased significantly from baseline in both groups. Energy intake, however, decreased significantly only in the intermittent group (-221.0 ± 108.3 kcal/d)
The second thing is that empaziflogin use changes your gut microbiata (after just 4 weeks!) and plasma metabolites (after 3 months).
After the 3-month treatment period, empagliflozin increased the levels of fatty acids, fatty acyls, organic acids, phosphosphingolipids, and other metabolites such as maslinic acid but reduced the levels of amino acids and derivatives, lipids, vitamins, sugar alcohols, and other metabolites such as uric acid […] We found a significant increase in the sphingomyelin and capric acid levels and a decrease in glycochenodeoxycholate, cis-aconitate, erythritol, and uric acid in the empagliflozin group but not in the metformin group
We found that the richness (observed ASVs) and diversity (Shannon index) of the gut microbiota significantly increased in the empagliflozin group but not in the metformin group . The aPCoA of Bray-Curtis distance demonstrated that the gut microbiome of the patients showed a significant shift after 4 weeks of empagliflozin treatment and then remained relatively stable
The clinical benefits of both empagliflozin and metformin are related to altered plasma metabolites; plasma metabolite alterations, in turn, are associated with changes in the gut microbiota of patients. Empagliflozin modified plasma metabolites and gut bacteria related to clinical parameters, including blood glucose levels, inflammatory factors, and CVD-related factors, whereas metformin treatment was associated only with changes in blood glucose levels and body weight-related modifications in plasma metabolites and gut bacteria.
The above tells me that potentially, I could dose empa the following way to get most of its benefits:
- take it faily for 1 month. This would results in potential weight loss, and also in enriching and diversifying my gut microbiata
- take it intermitently after 1 month, maybe once a week. This would at least lead to weight maintenace, and more importantly help maintain gut microbiata diversity.
It’s an open question how long those change to the microbiome stay after being on empa for some time, but to me it points to another another criterion I’ll start using for anti-agin intervention: the frequency of the dosage. The less frequent, the better. We still don’t know what the optimal dosage of rapamycin is, but seems like at most once a week is a good start. It could be that once a month is also OK, who knows. Other interventions that last a long time:
- flagellin immunization (3 years and counting): Two Year Update on a Study of One with Flagellin Immunization to Adjust the Gut Microbiome – Fight Aging!
- FMT (6 months): Three Years of Gut Microbiome Data for Flagellin Immunization and Fecal Microbiota Transplantation – Fight Aging!
I finally feel confident enough about my understanding of gut microbiome testing to order one. I plan to do one soon, while still on rapamycin, and a couple more when I start using empa.
6 Likes
Nice report, thank you for posting! You ask for any numbers that stand out…
I suspect that your improved RDW (%), 13.5 in Oct 2022 to 12.5 in Jan 2023, has had the single largest impact on your epigenetic test and your improved biological age. I had a very similar improvement post Rapa use. Try swapping the 2022 RDW number into your 2023 numbers and you will probably see a significant negative change in your biological age.
Yes, I agree that the current epigenetic tests are raw but the RDW measurement seems to be a decent indicator. Here’s a paper discussing RDW% Genetic and epigenetic regulation of human aging and longevity - ScienceDirect
And a blog by Michael Lustgarten that explains RDW% metrics and effect.
2 Likes
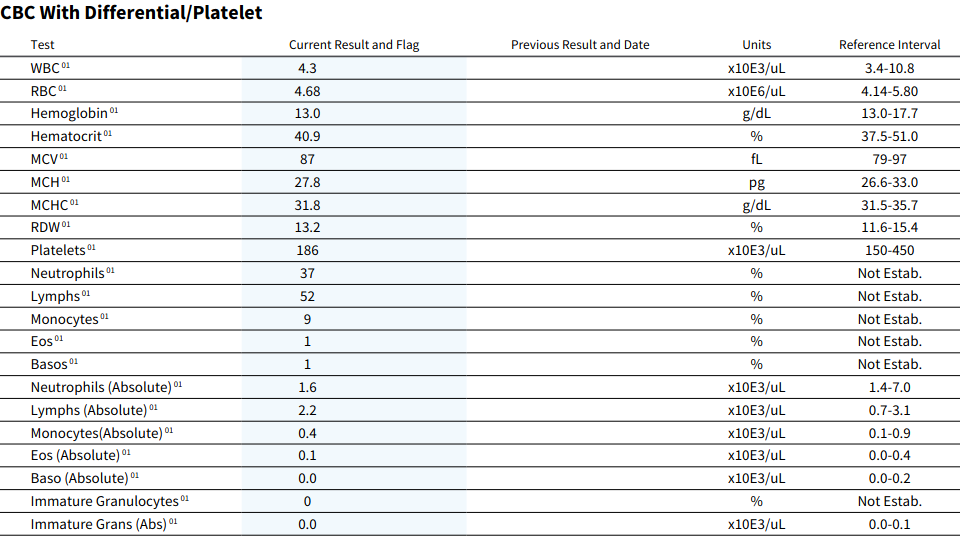
Here is a partial update based on some blood work I did earlier:
Blood work:
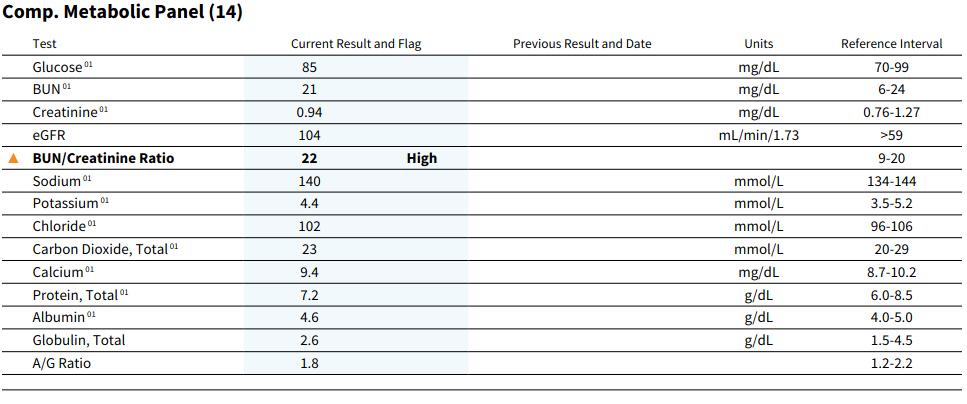
Metabolic panel:

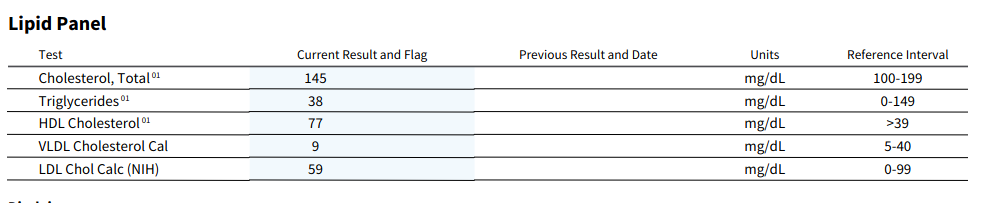
Lipids:
Phenotypic age regressed a little:
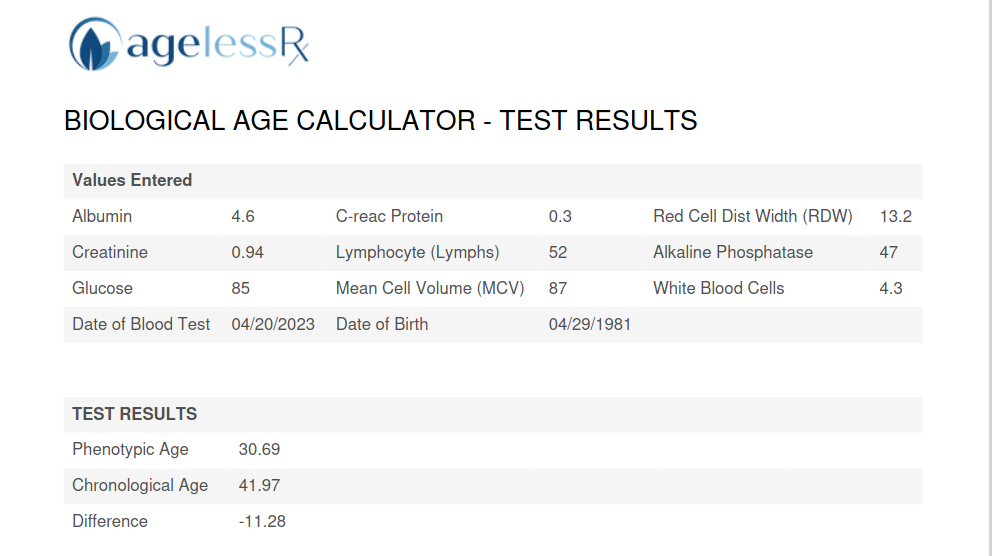
This is over a 3-month period where I am at the following dosage:
- 6 mg/week of rapamycin
- 10mg/day statins
- 70k mcg B12 once a week
- 50k IU/week vitamin D
- 2.2g fish oil
So at worst, 6mg/week of rapamycin doesnt seem to yield any improvements that I can see.
2 Likes
Do you take D3 once a week rather than D3/7 every day?
Do you take D3 once a week rather than D3/7 every day?
Once a week
My husband just got his sirolimus (Rapamycin ) blood lab results
Current results 0.9 ng/ml
Reference point is 3.0 to 20.0 so very low after 4 th cycle of 3 months on and 1 month off of 3 mg per week.
Not a very encouraging result
2 Likes
What day was the blood test done after he took the rapamycin? That sounds like a trough measurement at the end of the week just prior to taking another dose.
He takes Rapam on Sundays and you are correct, he took his blood labs on the Friday , he will take another test in a month one day after dosing, thank you for that information
1 Like
As a trough measurement that is exactly where he wants it - under 1ng/ML. So it sounds like the schedule from a dosing / blood level standpoing and timing point is working ok for him.
The whole idea of testing earlier after dosing - e.g. 1 to 4 hours after, or even a day after as you’ve suggested, is very much debated here in our forums and its more of a “nice to know” type of thing vs. something actionable that you can work from. The Cmax (highest blood level) of sirolimus is sometime around 1 to 3 hours after dosing, and of course varies person to person. Its interesting to know the peak blood levels of sirolimus primarily because there are research studies that suggest that higher doses / blood levels penetrate the blood barrier level better… see: Rapamycin and the Issue of Getting Through the Blood Brain Barrier
But the peak is a really sharp peak if you look at the blood level graphs as shown in this thread: How to get a Rapamycin (sirolimus) Blood Level Test
So - its difficult to say how accurate any measure of peak blood levels is, given how quickly it drops off.
Anyway - just a little background so you can understand the issues related to blood sirolimus testing.
7 Likes
Yes, that was very helpful information and link
Thank you
1 Like
Strangely enough, if you follow carnivore diet adherents, they argue that it’s not the lipidoemia that causes damage and plaque formation in blood vessels.
1 Like
Good results. Ageless Rx appears to use the PhenoAge algorithm developed by Morgan Levine. Same parameters. Spreadsheet can be found free online and downloaded. You can also find a PubMed paper by her on this. It seems to be fairly good. Gives most weight to RDW, which dropped for you from 13.5 to 12.5. Your MCV is also good. My RDW has moves around a bit and seems to be based on how well I stick to my health routine (I’m not on Rapa yet). Didn’t see your Vitamin D, B12, or Omega 3 blood results if you ever like to share. Excellent insulin. Thanks again for posting all your data.
1 Like
I guess this is a reply to an April '23 post. Still…
That’s a lot of vitamin D. I’m curious about your rationale for taking so much and for taking it once/week rather than every day? There are animal studies showing too much can actually promote arterial calcification. I’m not sure your dose is in that range but if it were me I’d spread it out daily over the entire week and reduce the dose to no more than 4000 IU/day. If nothing else I’d encourage you to read up on high dose vitamin D and it’s potential side effects. Depending on where you live you may not need any at all.
He takes 50,000 IU per Week, not day. That comes out to about 7,000 IU daily. I take 10,000 IU daily which is 70,000 IU per week. I still have barely sufficient levels (30) where 29 is deficient. I’m aiming for at least 40.
2 Likes
Wow, when I took 10k daily my levels got to 95!
1 Like
D3 in oil is more bioavailable.
3 Likes
95 would be good. I hope to get there. Honestly I’ll take anything above 40.