@brandy111 Good point! Sirolimus absorption has been a trouble spot and why compounding versions can have issue vs. commercially available.
Dr. Mannick’s pod cast brought up many good points including the comment about mTOR modulation and how it changes with aging - younger people turn off mTOR when they fast (assuming she is talking about when they sleep) and older people do not do this modulation as much. Taking your mTOR blocker of choice at night when it has a peak may make sense?
Trying to mimic the mTOR modulation of the young is one approach, but it appears that periodic blocking of mTOR of younger (mice) may have even a better effect on longevity. This may create a question of trying mimic younger mTOR modulation vs. Supraphysiologic (more blocking than is normally seen than just by being young).
Observationally, it seems most of the experts that try the every 2 week (high) dosing, go back to the weekly dosing - Attia, Green, Dr. B.
After having tried different doses from 1 - 6 mg +GFJ (4-6 mg was every two weeks), I think my sweet spot is 3 mg + GFJ weekly. I may try a higher dose every now and then. Thanks for all the discussion and information.
Hey Chris… you have come to where I have… 2mg and GFJ…I should be getting a 12 mg dose based on my GFJ reaction. Seems to be working well… after months of 36 mg… where I felt wonky…everything seems pretty good across the board now… muscles, workouts, weight maintenance mental alertness. I will do a new blood panel in a few weeks… and post it. Think 2mg and GFJ is my sweet spot… also I do continuous rapamycin…no breaks.
That’s not quite accurate. First, the weekly mouse studies postdated Mannick’s human trials.
Second, Mannick’s first trial, they tried 0.5 mg everolimus daily, 5 mg weekly, 20 mg weekly. 5 mg weekly was as effective as the others with fewer side-effects.
In the Phase 2A, they used 0.5 mg of everolimus daily, 0.1 mg of everolimus daily, 10 mg of the catalytic inhibitor RTB101 (previously known as BEZ235) daily, or a combination of 0.1 mg of everolimus and 10 mg of RTB101 daily. Based on the primary outcome (vaccine response), only the combination succeeded; if you spelunk around in the paper, I think you could make the case that all the everolimus-containing protocols had some effect.
In the Phase 2B, they used RTB101 5 mg daily or RTB101 10 mg daily in part 1 and RTB101 10 mg daily, RTB101 10 mg twice daily, or RTB101 10 mg plus everolimus daily.
Again pointing to the fact that more is not better. The max dosage without undesirable side effects as once postulated by Dr.Blagosklonny is dead as far as I am concerned.
[ desertshores]
Again pointing to the fact that more is not better. The max dosage without undesirable side effects as once postulated by Dr.Blagosklonny is dead as far as I am concerned.
Well, except that in the rodent longevity studies, it’s very clear that the higher the dose the better — and in nearly all of those, the animals get their rapa several times a day, every day, in their food. I think it’s a serious question whether anyone taking 5-10 mg rapa or everolimus weekly is getting an effective anti-aging dose.
Yes, I am well aware of the more is better theory. This may be true for rats, mice, fruit flies, etc, but of course everybody knows that these studies don’t always translate to humans.
Humans have more genes in common with cats and dogs, than rats and mice.
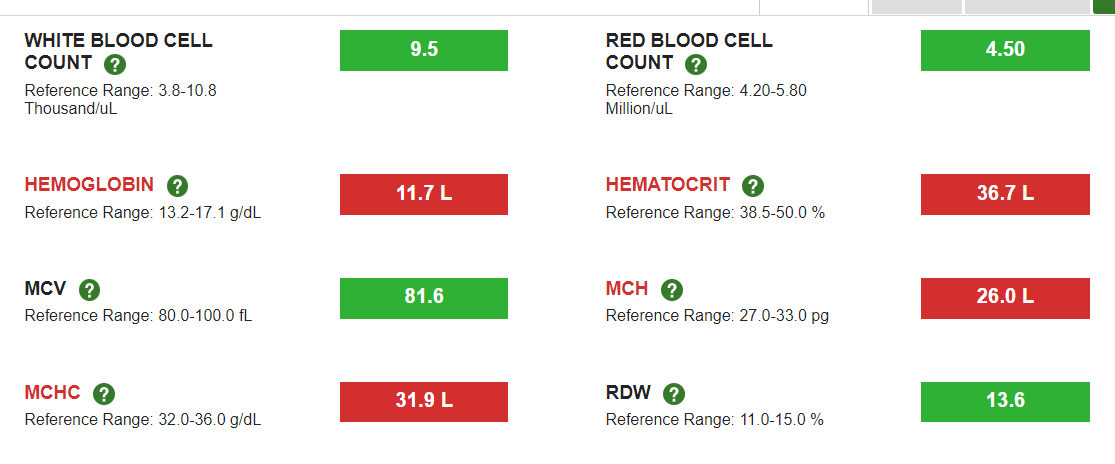
My own blood work over the course of ~15 months indicates that the high doses I have been taking are probably detrimental or at least not optimal. Many other forum members have reported worsening blood test numbers such as ferritin, MCW, etc. while taking rapamycin.
So no, I absolutely believe that there is an optimum dose and/or frequency for taking rapamycin.
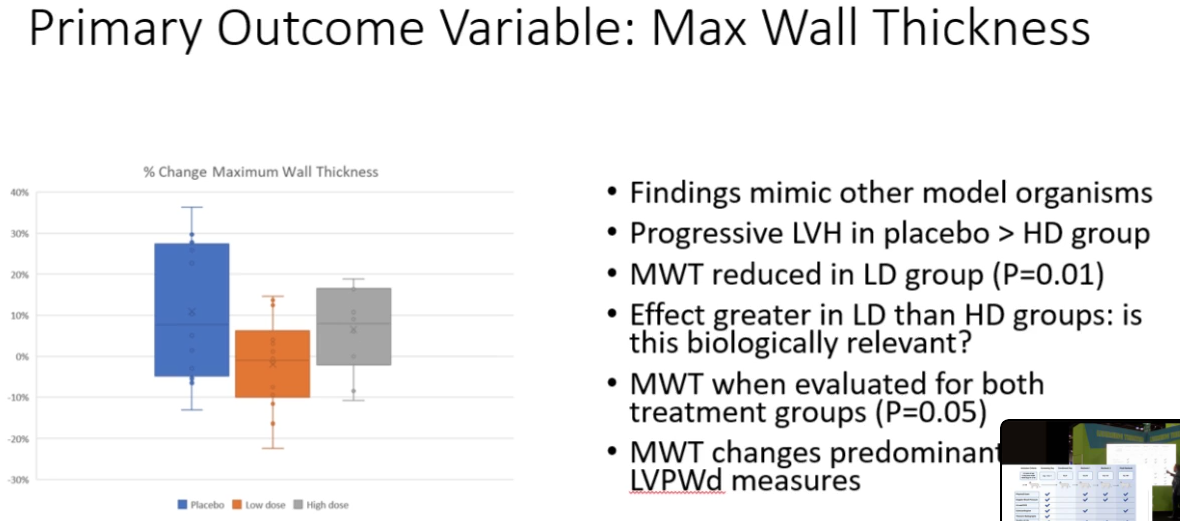
This study of cats being treated for hypertrophic cardiomyopathy indicates the best dose is not the highest dose.
I think the anecdotal reporting from forum members is beginning to give us a clue that higher doses are not necessarily more beneficial.
This video has be previously posted, but I won’t make you look for it.
“Understanding Feline HCM: Prognosis, Genetic Mutations and Emerging Treatment Options Dr. Joshua Stern - UC Davis”
The thing that pushes me to do a larger dose on occasion are the results from fasting studies. Fasting has different autophagic effects that are magnified the longer the fast goes on. Since Rapamycin is a fasting mimetic, I believe that the same could be true for Rapamycin use and maybe once or twice a year, a large dose with a longer washout period could be adopted. Sometimes variety is needed.
As an aside, I think fasting is additive to Rapamycin’s autophagic effects. My father, who does OMAD but not Rapamycin also experiences canker sores when he fasts with similar Rapa side effects.
Two things here. First, that’s narrowly true of cats but not dogs: humans share 90% of genes in common with cats, but 85% with rodents and 84% with dogs. Additionally, domestic catas have an exceptionally high frequency of disease-causing SNPs,
This relates to another misunderstanding you appear to have below.
Additionally, whatever other merits cats and dogs may have as experimental models, we don’t have any rapa lifespan studies in either species (yet). Absent that information, the cat and dog data are only of interest for hints of conservation, regardless of how closely-related they are.
The fact that you had more side-effects on higher doses does not mean that lower doses are more or equally effective. Depressing as it may be to contemplate, it may be that the doses required to meaningfully affect human aging are not achievable without unacceptable side-effects. Certainly translating the rodent dose-response studies raises that concern.
By definition there is an optimum dose and/or frequency for taking rapamycin. The question is how high that dose is and if we are even in the ballpark.
Something you may not realize is that hypertrophic cardiomyopathy is not the kind of cardiomyopathy that happens to some degree in all humans as a result of aging processes including blood pressure and cardiac amyloid, but is a genetic disease that is common in cats but rare in humans. It makes sense that a genetic disease of heart muscle overgrowth could be treated with a drug that suppresses a growth pathway, but that doesn’t necessarily tell us much about aging in humans unless they are unlucky enough to be genetically susceptible to the disease.
Aside from side-effects, which may or may not tell us anything about efficacy, what would you point to? Also remember that Joan Mannick says that nearly every person on placebo in her trials was subjectively certain he or she was on an anti-aging drug …
This forum is full of great information, but it’s also full of people who are imagining lots of “miraculous” effects from a few rapamycin doses (both in themselves and their dogs). I’m at 10mg rapamycin per week and haven’t seen any positive (or negative) effects at all.
I like the discussion, data presented and arguments for what makes sense on what dosing approach to use. All that being said, this is an evolving process that is very common in medicine. Hopeful animal data, long term human data probably needing many years to collaborate and in the mean time a discussion of balancing risks and benefits. Our safety data seems to be pretty good other than knowing what taking Rapamycin may do for extended periods of time beyond our current data set. (more applicable for the 20 year olds taking Rapa)
I have made this argument previously on this site, but I feel for myself, I need to see a positive for why I would take on the risk of an unknown. The risk of doing nothing is known, so not unreasonable for the argument of doing some approach even without a noted positive change. For now, I take Rapamycin for its Healthspan value(decrease of joint and muscle inflammation) and hopeful for its longevity value.
Doseage adjustment is awkward at best:
Feeling sick, mouth sore, bad labs = then wash out or decrease the dose.
Feeling good and stable labs = keep the same dose.
Not feeling as good as previous, bored with progress, wanting to get best optimal dose and normal labs - increase dose and or interval change.
@RapamycinCurious - has made some good points that none of our current approaches and or reasoning may have anything to do with optimal longevity dosing = best longevity dose could be with poor looking labs and side effects.
I do 3 - 7 mg / weekly without GFJ, trying night time dosing to enhance fasting mTOR effect and reading daily on what better options or reasoning is out there
What proof do you have that rapamycin has any efficacy? Other than side effects I have seen no positive effects on blood work, than Agetron’s miraculously positive benefits.
I you put “ferritin” into the question box you will see the forum members that are experiencing below or significantly low iron levels after taking rapamycin. Maybe this is why some forum members experience tiredness after taking rapamycin. It certainly is not good long-term, unless you think anemia is a good thing.
I will continue to take rapamycin in the future but that is based on some faith in animal studies, not because there is any proof it does anything in higher primates.
Just as an aside: Recent pictures and interviews with Dr. Allen Green don’t seem to indicate that it is having any significant observational benefits. He does in fact seem old and frail to me. This is not a criticism of Dr. Green, it is just a subjective observation.
I would tend to agree that a couple doses doesn’t make much of a difference. For me, it took 3 full months 90 days before I saw the 1st evidence of rapamycin doing something… which was at that point starting to remove the visceral fat about 15 pounds in weeks. Then the dysphagia…choking vanished. Then my strength started increasing 10 -15 pounds increases at gym every 3 months, skin started plumping up veins opened up.
Memory is the most amazing. I will be stuck on remembering a name or person… that I knew… . Pause… let my mind go blank… and bam… it appears… pretty amazing. Before Rapamycin, I would have to Google hints…to get it and then could move on.
On rapamycin 2 years and 8 months… I feel now the major miracles are done… lol. Just maintaining and keeping what I got back.
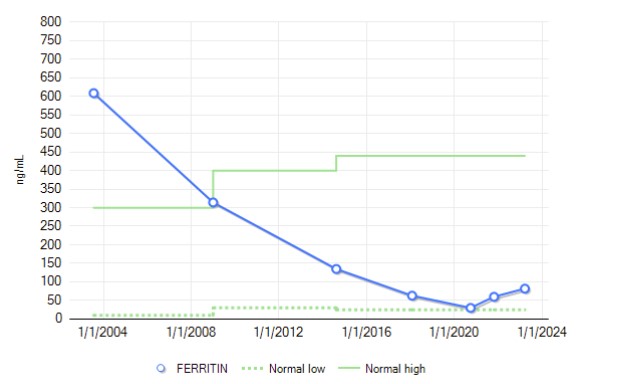
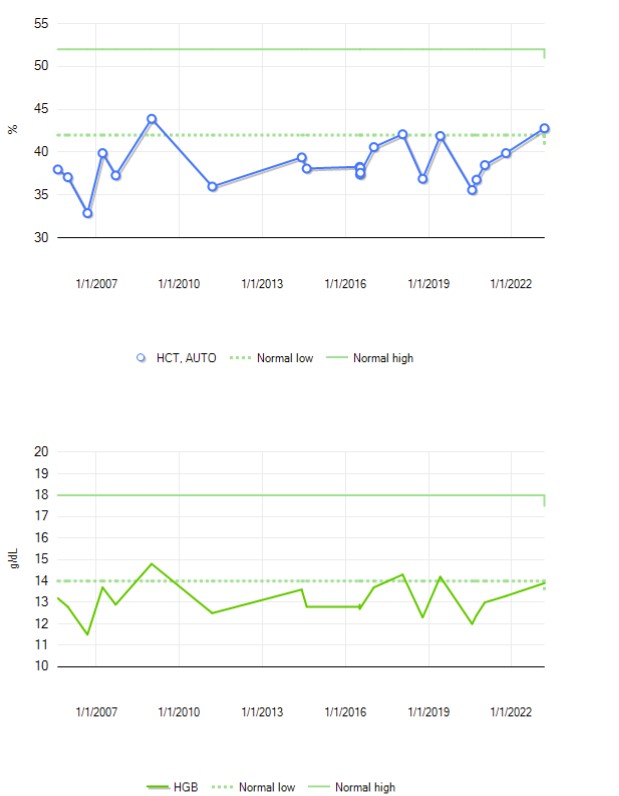
Interesting though, that over the last two decades, my ferritin level has dropped steadily from 600 to 30 (last reading 80), and yet presumably related markers have been utterly trendless during that same time period. So, not necessarily correlated for high values of ferritin.
Couple years ago, I was sure ferritin was headed to zero. Doc did not evince concern, said there’s other stores.
I think we can all say that the ITP results and other Rapamycin experiments have made a pretty good case for taking Rapamycin for health and longevity. The dog studies are also encouraging. So the question is how much do we take?
At 1-2 mg, some people experience side effects so Rapa has some effect at this point. However some do not. I would say this is too low of a dose for most.
3-5 mg seems to be a dose that packs a little more punch without too many side effects. For those preferring to play on the safe side, 5 mg and below seems to be pretty safe.
6-9 mg is where many of the longevity folk such as Dr. Attia and others are taking. A little bit more punch. This should be equivalent to 2-3 mg + GFJ.
10-20 mg seems to be the every two weeks schedule with a high peak at the beginning.
Then there are the true experimenters that do 20 mg+. They have shown us you can take this amount without too many bad side effects although this is where ankle swelling and some other side effects that are more major start cropping up.
Fortunately most side effects at any dose start reversing once dosing stops. The worst side effect is a bacterial infection which could be lethal if your immune system is too suppressed by Rapa. Please discontinue Rapa use if you have an infection or have surgery or major wound healing.
That seems to be a pretty good summary. Any modifications?
I think you misunderstand me. I am absolutely not sure that it will work in humans, and one of the reasons I’m in doubt is exactly because the animal studies that I agree are the core evidence around which everything else is just hints suggest that effective doses would be much higher than people are using now. As I said,