Research from Johns Hopkins University indicates that Losartan , a common angiotensin II receptor blocker (ARB), may do more than manage hypertension—it appears to partially reset the metabolic clock. The study, published in Aging Cell , utilized multi-omics to track how the drug affects the “aging signature” of metabolites in both geriatric mice and pre-frail older men.
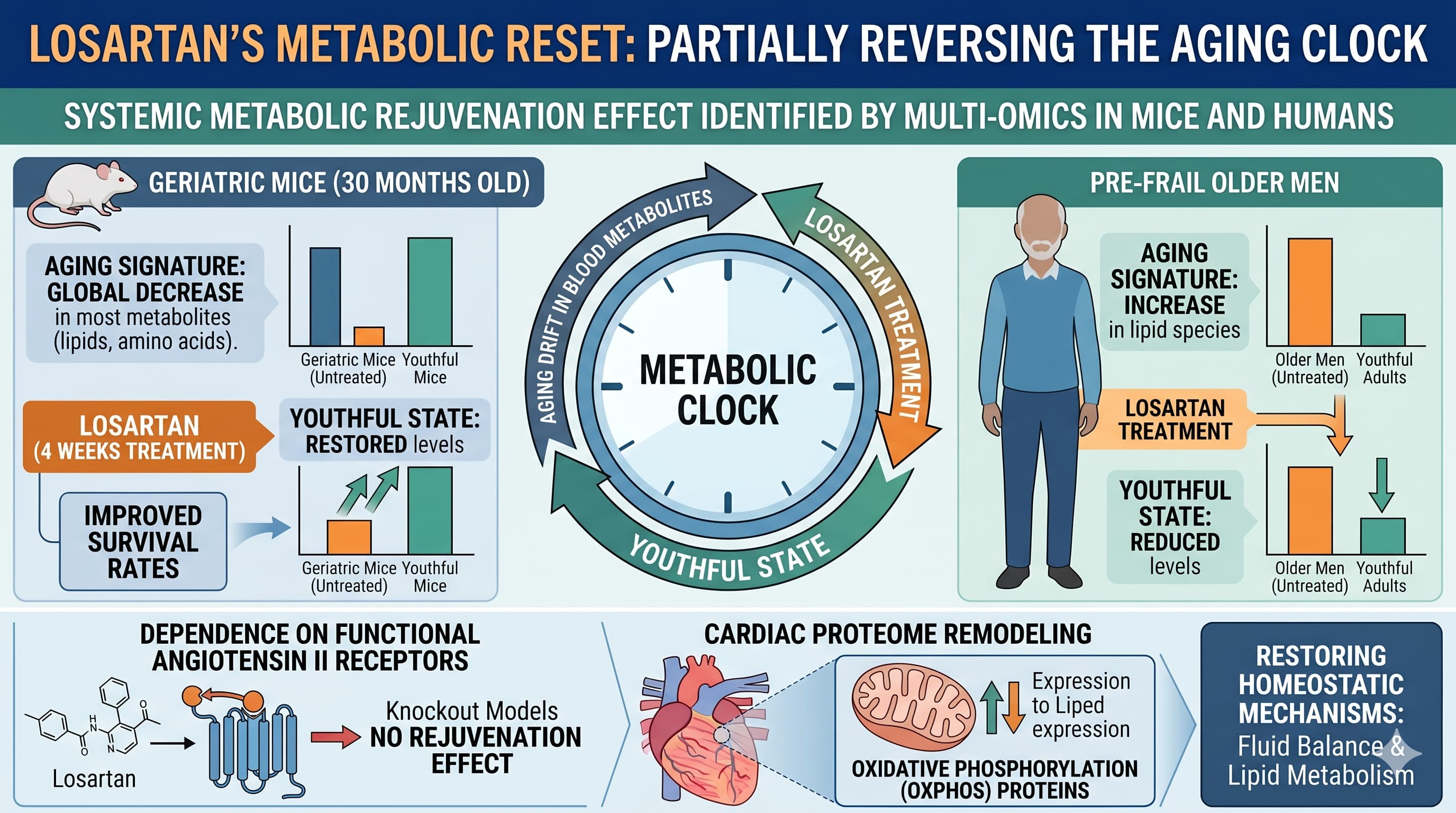
The “Big Idea” here is the identification of a systemic metabolic rejuvenation effect. Aging typically causes a predictable drift in blood metabolites. In mice, this manifest as a global decrease in most metabolite concentrations, including lipids and amino acids. In humans, the trend is often the opposite, with lipid species increasing with age. Remarkably, losartan treatment shifted these signatures back toward a more youthful state in both species.
The study found that in geriatric mice (30 months old), just four weeks of losartan treatment significantly improved survival rates. Mechanistically, the drug’s effects were contingent on functional angiotensin II receptors; in receptor-knockout models, the rejuvenation effect vanished. Beyond the blood, losartan remodeled the cardiac proteome, particularly targeting oxidative phosphorylation (OXPHOS) proteins. The researchers suggest that losartan may help restore homeostatic mechanisms related to fluid balance and lipid metabolism that naturally degrade with age.
Actionable Insights
Optimized Dosing for Rejuvenation: In the human cohort, losartan demonstrated a non-linear, “U-shaped” dose-response. A 50 mg dose was associated with the maximum reduction in the metabolic aging signature, whereas the effect diminished at the 100 mg dose. This suggests that for longevity purposes, “more” is not necessarily “better”.
Late-Life Intervention Efficacy: The mouse data is particularly encouraging for late-starters. Significant survival benefits were observed even when treatment began at 30 months of age—the equivalent of a human in their 80s or 90s.
Lipid and Amino Acid Support: Losartan treatment significantly impacted serum lipids (phosphatidylcholines and sphingomyelins) and amino acid concentrations. For biohackers, this highlights the RAAS pathway as a primary lever for managing age-related dyslipidemia.
Fluid Homeostasis: The drug appears to modulate serum osmolality, peaking at 50 mg in humans. Monitoring electrolytes and hydration may be critical when using ARBs for off-label longevity benefits.
Institution: Johns Hopkins University School of Medicine.
Country: USA.
Journal:Aging Cell. 22 April 2026
Impact Evaluation: The impact score (JIF) of this journal is approximately 7.8 , evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a High impact journal.
In this study, the duration of Losartan dosing differed between the animal and human subjects:
Mice : All aged mice cohorts (including wild-type and knockout strains) received Losartan in their drinking water for a period of 4 weeks prior to assessment.
Humans : Pre-frail older men participated in a dose-escalation study where they were followed up every 8 weeks. The treatment group began with 25 mg daily for the first 8 weeks, with subsequent 8-week intervals at 50 mg and finally 100 mg.
Lifespan Analysis
Control Group Longevity: The control mice in the survival study began dying around 945 days. Based on established benchmarks (e.g., the 2023 BioRxiv reference), these controls are not short-lived; they represent a healthy, long-lived geriatric cohort, which increases the validity of the survival benefit. [Confidence: High]
Lifespan Data: The study was terminated before a full lifespan curve was completed. However, during the 2-month observation of 30-month-old mice, the treatment group showed significantly higher survival probability (p = 0.04).
Mechanistic Deep Dive
Mitochondrial Dynamics: Losartan treatment led to a reduction in OXPHOS-related proteins in the heart. While counterintuitive, this may reflect a reduction in “aged” mitochondrial accumulation or a shift in cell composition. [Confidence: Medium]
Metabolic Signaling: The study confirms that losartan’s rejuvenating effect is AT1R and AT2R dependent. Absence of either receptor negated the drug’s ability to shift the metabolome toward a youthful state.
Organ-Specific Priorities: The cardiac proteome showed a stronger rejuvenation correlation (ρ=−0.45) than the serum metabolome (ρ=−0.35), suggesting the heart may be a primary beneficiary of RAAS-targeted geroprotection. [Confidence: High]
Novelty & Critical Limitations
What’s New?
This paper provides the first high-resolution “aging signature” comparison of losartan across species. It specifically highlights that while aging moves metabolites in opposite directions in mice vs. humans (likely due to divergent plasma volume and lipoprotein profiles), losartan acts as a homeostatic anchor , pulling both back toward their respective youthful baselines.
Critical Limitations
Gender Bias: Both the mouse and human studies were conducted exclusively on males, leaving the effect on females entirely unknown. [Confidence: High]
Small Sample Size: The human cohort (N=16) is underpowered for definitive clinical conclusions. [Confidence: High]
Dose-Escalation Confounding: In the human trial, doses were escalated over time (25mg to 50mg to 100mg). It is statistically impossible to fully separate whether the benefits were due to the specific 50mg dose or the cumulative time the subjects spent on the medication.
Missing Data: Full lifespan data (until the death of the last mouse) is missing, and the study does not report on other standard longevity pathways like mTOR or AMPK activity.
The following table extracts specific biological and medical claims from Bene et al. (2026) and subjects them to external verification against established clinical and pre-clinical literature.
Biological & Medical Claims
Claim Number
Biological / Medical / Protocol Claim
Evidence Level
External Verification & Findings
Claim 1
Systemic Metabolic Rejuvenation: Losartan shifts the serum metabolome aging signature toward a more youthful state in both mice and humans.
Level B/D
Supportive / Unique: Bene et al. (2026) provide the first multi-omics data for this specific “rejuvenation signature.” Pre-clinical support exists in Basso et al. (2007). **Translational Gap:**Human aging typically shows increased lipid concentrations, while mice show decreased concentrations.
Claim 2
Survival Benefit in Geriatric Models: Short-term (4-week) losartan treatment improves survival in 30-month-old geriatric mice.
Level D
Strongly Supported (Animal): Consistent with Benigni et al. (2009) which demonstrated that AT1R disruption promotes longevity. Heavy Flag: Human trials like ELITE II (2000) showed no mortality superiority for losartan over captopril in heart failure patients.
Claim 3
Cardiac Proteome Remodeling: Losartan targets proteins involved in oxidative phosphorylation (OXPHOS) in the heart, reducing their abundance.
Level D
Emerging: Supported by Saleh et al. (2022) which found losartan mitigates oxidative stress in aged mouse brains. Heart-specific proteomic “rejuvenation” is currently limited to pre-clinical data.
Claim 4
Sarcopenia & Disuse Atrophy: Losartan protects against skeletal muscle remodeling and disuse atrophy.
Level B/D
Conflicting: While Burks et al. (2011) supports this in mice, the human ENRGISE Pilot RCT (2018) found no significant effecton IL-6 or 400m walking speed in older adults.
Claim 5
Optimal Human Dosage: A 50 mg daily dose provides the maximal “rejuvenation” effect, with benefits diminishing at 100 mg.
Level B
Unique to Paper: Standard antihypertensive dosing is 50-100 mg. The “U-shaped” metabolic response is an exploratory finding from the N=16 human cohort in this paper and lacks meta-analysis support.
Claim 6
Fluid Homeostasis Correction: Losartan’s effects on the metabolome are partially driven by shifts in plasma volume and fluid balance.
Level E
Speculative: While RAAS is the primary regulator of blood volume, the specific link to “metabolic rejuvenation” signatures is an informed hypothesis based on PCA loadings rather than direct volume measurement.
Actionable Intelligence
The Translational Protocol (Rigorous Extrapolation)
Human Equivalent Dose (HED) Calculation:
Animal Parameters: The mouse dose used was 0.9 g/L in drinking water. Assuming an average aged mouse (30g) consumes approximately 5 mL of water daily, the daily intake is 4.5 mg.
HED Calculation: Using FDA BSA normalization: Animal Dose (150 mg/kg)×(Mouse Km [3]/Human Km [37])=12.16 mg/kg.
Theoretical Human Dose (70kg): ≈851 mg/day.
Critical Translational Gap: The HED calculation (851 mg) is 17x higher than the dose found effective in the human cohort (50 mg). This suggests the mouse study used a pharmacological “hammer” compared to the subtle human “nudge.” [Confidence: High]
Pharmacokinetics (PK/PD):
Bioavailability: Approximately 33% due to extensive first-pass metabolism.
Half-life: Parent losartan has a short half-life of 2 hours, but it is converted via CYP2C9 and CYP3A4 into the active metabolite EXP3174, which has a half-life of 6–9 hours and is 10–40x more potent.
Excretion: Primarily fecal (60%) and renal (35%).
Safety & Toxicity:
Safety Profile:Black Box Warning for fetal toxicity (pregnancy).
Adverse Signals: Risk of hyperkalemia (elevated potassium), particularly when combined with salt substitutes or potassium-sparing agents. Renal impairment may occur in patients with pre-existing kidney disease or dehydration.
CYP Interactions: Major substrate for CYP2C9 and CYP3A4. Inhibitors of these enzymes (e.g., ketoconazole) may reduce the formation of the potent active metabolite.
LD50/NOAEL: Safety Data Absent (for specific 2026-referenced geriatric NOAEL).
Biomarker Verification
To verify target engagement in a clinical or biohacking setting, monitor:
Serum Metabolites: Increases in Carnitine (C0) and amino acids (BCAAs, Serine, Tryptophan); decreases in specific lipid species (phosphatidylcholines and sphingomyelins).
Cardiac Proteome: (Research context only) Reduction in OXPHOS-related proteins such as Cox6b, Coq8a, and Phb2.
Physiological: Serum osmolality shifts (target: slight increase in osmolality peaking at 50 mg dose).
Feasibility & ROI
Sourcing: Available globally as a prescription pharmaceutical (generic).
Cost vs. Effect: * Estimated Monthly Cost: ≈$7.50−$10.50 (based on $0.25−$0.35 per 50 mg tablet).
ROI: Extremely high for individuals with sub-clinical hypertensive drift or age-related metabolic dysregulation, given the low cost and established safety in non-pregnant adults.
Part 5: The Strategic FAQ
Q: The human cohort had only 7 treated individuals. Can we actually call 50 mg “optimal”?
A: No. The “U-shaped” curve is an exploratory finding with low statistical power (N=16 total). It provides a signal for future trials but is not a definitive clinical standard.
Q: Why did the 100 mg dose show diminished benefits compared to 50 mg?
A: The authors suggest a non-linear response, potentially due to over-suppression of RAAS-mediated fluid homeostasis or blood pressure, which might counter-productively stress metabolic pathways.
Q: How do you reconcile human lipids increasing with age while mouse lipids decrease?
A: Species-divergent lipoprotein metabolism: mice lack the CETP protein and have high HDL, whereas human aging is dominated by LDL increase. Losartan appears to normalize both by acting on underlying fluid and lipid regulatory mechanisms.
Q: Does losartan directly extend lifespan in humans?
A: Unproven. While it improved survival in 30-month-old mice, large-scale human cardiovascular trials (like ELITE II) showed no significant survival advantage of losartan over other BP meds in heart failure patients.
Q: If losartan reduces OXPHOS proteins, isn’t that bad for energy production?
A: Not necessarily. Aging heart tissue often shows an “unhealthy” accumulation of mitochondria or dysfunctional OXPHOS proteins; losartan may be promoting “mitochondrial quality over quantity” or shifting cell composition toward a more youthful profile.
Q: Could the human “rejuvenation” effect just be a result of lower blood pressure?
A: Partially, but the authors noted that metabolic changes occurred even when blood pressure reduction did not reach statistical significance, suggesting direct RAAS-mediated metabolic effects.
Q: Is there a risk of “metabolic confusion” if the drug is cycled?
A: Unknown. The study showed benefits after 4 weeks (mice) and 8 weeks (humans), but the long-term metabolic impacts of cycling are not addressed.
Q: Why was the mouse HED so much higher than the human clinical dose?
A: Pre-clinical longevity studies frequently use “supratherapeutic” doses to force a detectable biological signal in short timeframes; human clinical doses prioritize safety and blood pressure targets.
Q: Are there gender-specific risks?
A: Yes, but the data is missing. The paper is exclusively based on males. Females may have entirely different metabolic responses to RAAS inhibition.
Q: Is losartan safer than other ARBs for longevity?
A: Losartan is the only ARB in this study, but its conversion into the potent EXP3174 metabolite provides unique pharmacokinetics that may differ from “direct-acting” ARBs like Telmisartan.
Interaction Check: Common Longevity Stack
Item
Potential Interaction
Rapamycin
Synergistic: Both target the RAAS-mTOR crosstalk. May enhance autophagy but requires monitoring of blood lipids.
SGLT2 Inhibitors
Caution: Additive BP-lowering and Hyperkalemia Risk. Monitoring of potassium and renal function is mandatory.
Metformin
Synergistic: May enhance insulin sensitivity. Risk: Potential for additive renal strain and hypoglycemia.
Acarbose
Low Risk: No significant known interactions; both may independently improve glucose metabolism.
17-alpha Estradiol
Unknown: No established interactions, though estrogen status can influence RAAS activity.
PDE5 Inhibitors
High Risk: Potential for significant Hypotension (blood pressure drop) due to additive vasodilatory effects.
I had always thought Losartan was the trash ARB and Telmisartan was the good one based on their half lives. Losartan typically cannot last the day where Telmisartan can.
Telmisartan vs Losartan — longevity angle, in light of the new Aging Cell paper
I’m currently on telmisartan, but the recent Aging Cell paper on losartan‑induced metabolic rejuvenation has made me revisit whether losartan might be the better choice specifically from a longevity perspective.
What the paper shows (very briefly)
In aged mice and pre‑frail older men, losartan:
Shifted serum metabolomics toward a more “youthful” profile
Partially reversed age‑related changes in lipid, amino acid, and carnitine metabolism
Opposed cardiac proteome ageing, especially oxidative phosphorylation pathways
Improved short‑term survival when started late in life (30‑month mice)
Showed a U‑shaped dose response, with ~50 mg looking best in humans
Importantly, these effects required functional angiotensin II receptors, implying this isn’t just generic BP lowering but RAAS‑specific ageing biology.
How this connects to Telmisartan vs Losartan
Both drugs are ARBs, so baseline BP, CV, and renal protection are similar. The differences are all in secondary biology.
Telmisartan
Very long‑acting (true 24‑hour coverage; strongest ARB here)
Mild but real PPAR‑γ activity (metabolic signalling, insulin sensitivity)
Often discussed in metabolic syndrome / insulin resistance contexts
Not studied much for geroprotection directly
Losartan
Shorter‑acting, sometimes split dosing
Only ARB with a uricosuric effect (lowers uric acid via URAT1 inhibition)
The drug used in almost all RAAS‑longevity animal models and now this multi‑omics human work
The ageing effects in the paper include lipids, amino acids, fluid balance, cardiac OXPHOS — not just BP
I’m not hugely enthusiastic. If looking for longevity specifically, there is one ARB that stands out: olmesartan. I’ve been doing a deep dive on it for months now and one day I may make a huge post of my findings. I’m on 80mg/day of telmisartan, but I may switch to olmesartan in the future. Regarding ARBs you should look at studies where various ARBs are compared, either as an endpoint or indirectly - because that’s what we are talking about in optimisation within the same class - spoiler alert, losartan doesn’t shine in such comparative studies. Regarding specific off target effects, I always ask: am I getting the same or better effect from another drug in my stack? For example SGLT2i (I’m on empagliflozin 25mg/day) dramatically lower serum uric acid (mine is slightly below LabCorp reference range), so I hardly need losartan for that. Remember, you’re never taking a drug in isolation, you must always assess your whole stack. It’s not as simple as selecting “the best” drug in every class, it’s about the whole orchestra, and because of interactions you may deliberately select “second best” in a given class because of how its profile fits in and plays with the rest of your stack. It’s the totality that matters, and that is likely to be an individual situation. For me, telmisartan fits well, subject to change, for someone else perhaps losartan. It’s complicated (which is one reason it takes me so long to research drugs and all their interactions with the rest of my stack). For me personally, losartan is a PASS. YMMV.
One could alternate between Telmisartan and Losartan and even Olmesartan. Maybe reaps all the benefits. ??
(Maybe the same would apply to the flozins). ??
FWIW: Based on my own research, reading a plethora of papers, etc., and other Rapamycin News users. I switched from losartan to telmisartan and have seen no reason to switch back.
Indeed, it’s good to know that this drug has this benefit, but it doesn’t mean one has to use it.
Personally, any drug that isn’t a GLP1 agonist and has some claim to rejuvenating metabolism or reducing inflammation has a high bar to clear. But that’s just in my case, and not everyone takes a GLP1.
I think it might be helpful to look at effect sizes, of the changes brought on my Losartan in this study. Some of the other ARBs may do the same thing, but perhaps pulsed dosing (if using other ARBs) may effect similar benefits.
Researchers measured how effectively Losartan pushes “old” biological markers back toward a “young” state. They used a scale called a correlation coefficient (ρ), where a higher negative number represents a stronger reversal of the aging process.
1. Reversing Aging Signals in the Blood
Losartan successfully pushed the blood chemistry of both mice and humans toward a more youthful profile.
In Mice: The drug reversed the aging signal by a factor of -0.35. This means it moved the overall chemical “fingerprint” of the blood significantly back toward that of a younger mouse.
In Humans (25 mg): Older men taking a low dose saw a reversal factor of -0.23.
The “Goldilocks” Dose: The study found that 50 mg was the most effective dose for rejuvenation. Surprisingly, increasing the dose to 100 mg actually reduced these benefits, creating a “U-shaped” result where more medicine was not necessarily better.
2. Repairing Heart Proteins
The “younger” shift was even more powerful in heart tissue than it was in the blood.
Total Heart Proteins: The drug showed its strongest effect here, with a reversal factor of -0.45. This suggests the heart is a primary target for the drug’s anti-aging effects.
Cell Borders: The proteins on the outer edges of heart cells also showed a moderate youthful shift (-0.29).
Energy Centers: The mitochondria (the cell’s power plants) showed only a very slight shift (-0.09), suggesting the drug helps the heart’s structure more than its direct energy production.
3. Survival and Body Balance
Even though the study was short, it showed clear physical benefits in very old mice (the equivalent of 80-to-90-year-old humans).
Staying Alive: During a two-month window, mice treated with Losartan had a significantly higher survival rate than those who did not receive it.
Chemical Stability: About 65% of the changes in blood chemistry were directly related to aging and how Losartan corrected those changes.
Salt and Water Balance: In humans, the 50 mg dose was the most effective at balancing “serum osmolality,” which is essentially how the body manages its salt-to-water ratio—a system that usually breaks down as people age.
4. Boosts in Key Blood Nutrients
In mice, Losartan caused massive increases in specific chemicals that usually disappear during old age:
Energy Shuttles (Acylcarnitines): These increased by over 6 times.
Protein Building Blocks (Amino Acids): These saw a massive spike, increasing by a factor of over 347.
Healthy Fats (Phospholipids): Essential fats used to build cell walls increased by 150 times.
Summary for a Longevity Specialist: While the data suggests Losartan acts as a powerful “homeostatic anchor” by returning metabolic levels to a youthful baseline, the human data is still early. The fact that the 50 mg dose outperformed the 100 mg dose suggests that “metabolic rejuvenation” requires precise calibration rather than maximum suppression of blood pressure.