Not early enough. I’m not sure what the ideal age is to start rapamycin but I would think around 50, but it might be sooner.
I’m 81 and I didn’t feel any difference after taking rapamycin for a few months, but a skin condition I had for many years cleared up. Many report a reduction in aches and pains.
Not medical advice, but you might want to look into Acarbose which many here are taking to control glucose spikes.
2 Likes
I am already reading up on Acarbose.
True fully, I did not have any aches and pains, but I was never into any kind of real physical activity that would cause aches or pains.
I have started walking and doing 30 minutes daily exercise program.
I now, realize how important exercise is to one’s overall health.
Thanks, and appreciate all your post, they are informative.
2 Likes
CaptnJack, I have yet to notice anything specific with rapamycin other than a noticeably higher A1c test, and higher glucose spikes 1 and 2 hours after meals. I am aware of a colleague who had a leg amputated years ago because of uncontrolled blood sugar levels. So, like you, I pay attention to those high sugar levels and so far try to control them with diet. If you can’t do it with diet, definitely try Acarbose or some other alternative.
1 Like
I am currently controlling the glucose with Metformin and my last blood test fasting the level was 99 and one before that was 103. So even
with Metformin and a low carb diet my levels are barely acceptable.
Getting another blood test next Tuesday a week after taking the rapa.
So will see if there is any change that could be the rapa intake.
Hope not.
I’m sure you’ve read about Empagliflozin. But, if not, it may be something else to research on this site and elsewhere.
2 Likes
Yes aware, but I have not really researched it yet.
On my list though, a long with Acarbose.
" my levels are barely acceptable"
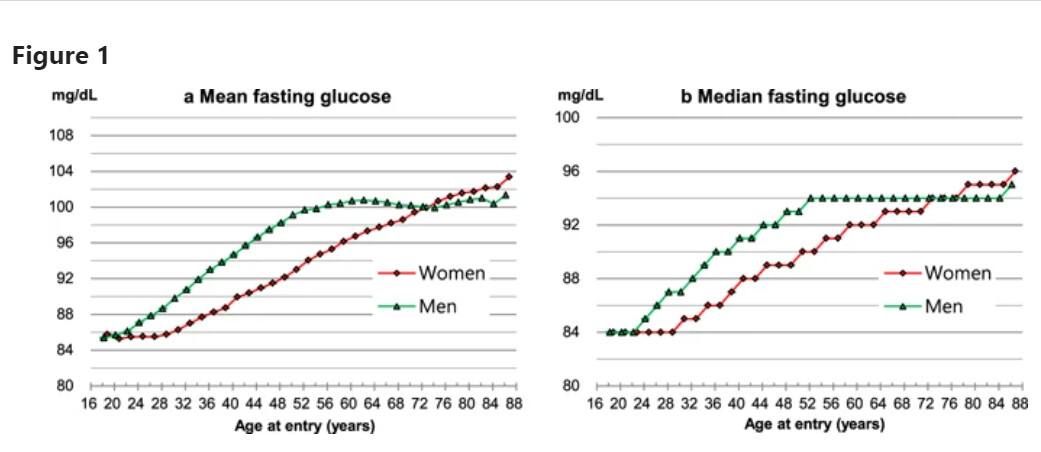
Well, that does have something to do with your age.
This chart shows the age-related association.
My doctor would probably think you are doing okay.
2 Likes
It is the Metformin and the low carb diet that is keeping it as low
as it is, but it is working. Will be interesting to the levels wen the
only change is the addition of rapa.
With me, the higher the dose I took the higher my lipids, but for one exception they were all still pretty good.
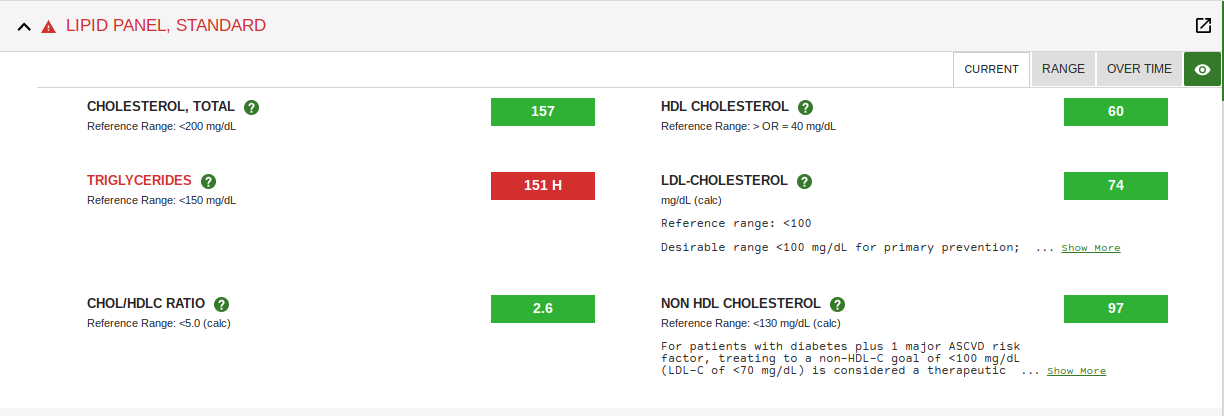
I am not particularly concerned about my higher lipid levels, but I trying to bring them down a tad.
3 Likes
My last blood test in Jan this year the results are in line with yours except HDL was 46 and LDL was 76.
So looking forward to the Tuesday test.
1 Like
Very well put. The older one is, the more one has to experiment at the higher doses to see what is tolerable and without unwanted side effects. Because of surgery I have been off rapamycin for over 3 weeks. Will soon do a blood test for rapa level, then re-start rapa and gradually build up dosage before repeating the test. I’m assuming that rapa (Sirolimus) is completely cleared after a few weeks of abstinence, but does anyone know for sure?
1 Like
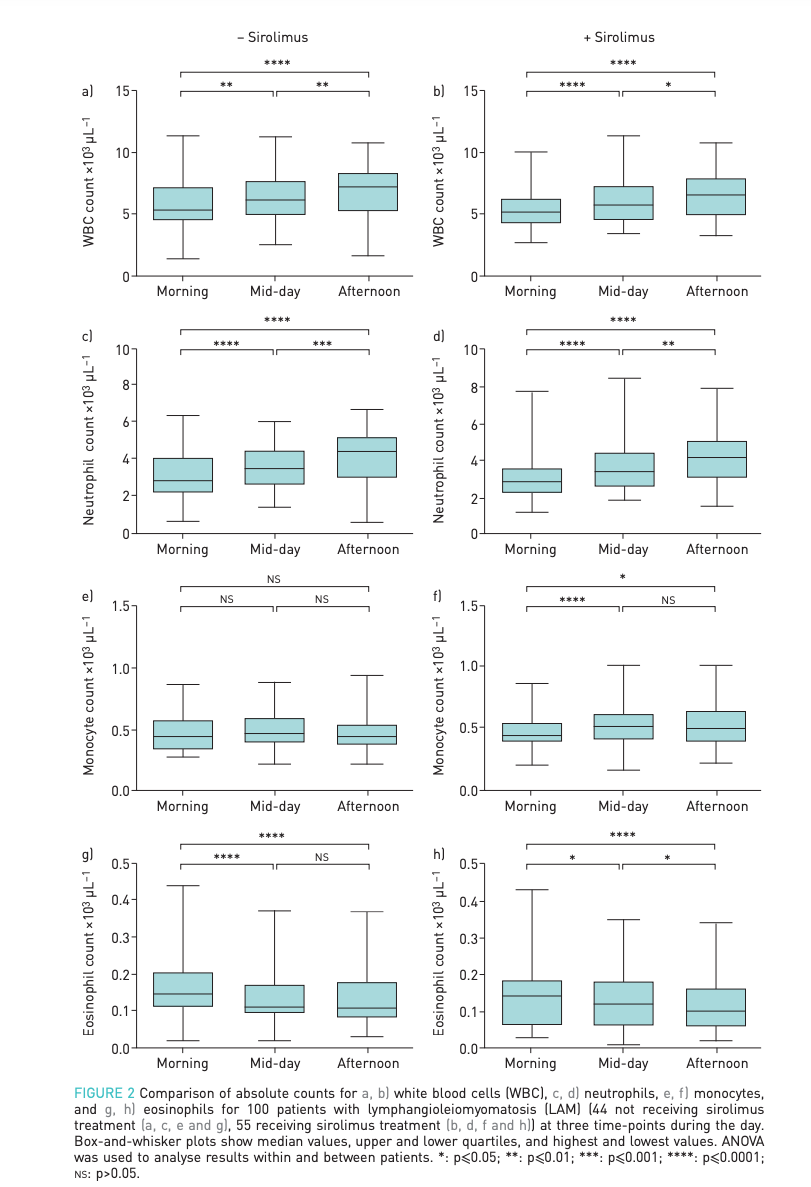
Here’s an interesting paper referencing the timing of the actual blood draw impacting immuno markers results.
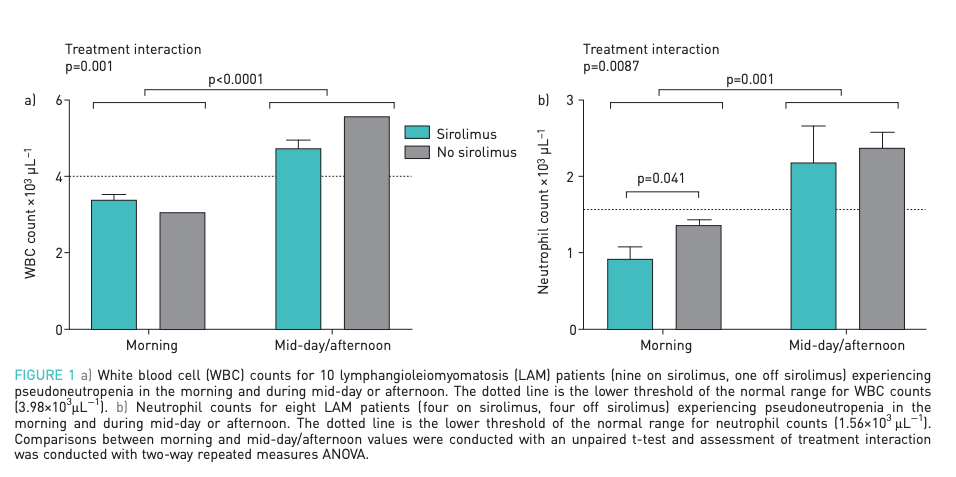
Pseudoneutropenia in lymphangioleiomyomatosis (LAM) patients receiving sirolimus: evaluation
in a 100 patient cohort
"Diurnal variation in white blood cells (WBC), particularly neutrophils, is well-described [1]. WBC levels are lower in the morning and increase through the day [1, 2]. Drugs with immunosuppressive effects, such as sirolimus, may further lower WBC counts. We report here a patient with LAM (female, age 53 years) receiving sirolimus who presented in the morning (06:00 h) with low WBC and neutrophil counts (3.18×103 µL−1 and 1.54×103 µL−1, respectively).
Previously, neutropenia caused the primary physician to decrease the dose of sirolimus. Repeat of the cell counts later in the day showed an increase in WBC and neutrophil counts by 42% (4.53×103 µL−1) and 88% (2.91×103 µL−1), respectively. These WBC and neutrophil levels would not warrant modification of the sirolimus dose."
5 Likes
Quick follow up here, I’ve had my HbA1C result after stopping rapa for 2 months and it came back at 5.3. So the single 8mg dose every 12 days seemed to be the culprit of my quite high (6.2) HbA1C (considering my age and fitness level stated in my original post).
1 Like
Hba1c assumes a red blood cell life of 120 days. This can be misleading because some poeple have longer or shorter lived red blood cells which throw off the average. Just thinking, could Rapamycin have an effect on the life span of red blood cells? is their any info on this?
From studies it seems that diabetics, or those prone to diabetes, have a more extreme glucose response to rapamycin.
Any family history of diabetes?
Maybe try a CGM for a couople months to see if that average corrospnds with the Hba1c reading. Also you can get a OGTT. they are avalable at life extension.
Newbalance, That’s an excellent question. I would like to know the answer to that question too because my HbA1c test also went up (5.3 to 5.6) while using rapamycin. Could an altered red blood cell lifespan affect the HbA1c test? I don’t know.
However, my thought is that there is no lifespan effect of rapamycin on red blood cells because my intermittent blood glucose tests also showed a significant rise while using rapamycin which tends to correspond with a higher HbA1c test.
2 Likes
Have you seen this paper?
Fasting and rapamycin: diabetes versus benevolent glucose intolerance
Puzzlingly, rapamycin can induce insulin sensitivity, but may also induce insulin resistance or glucose intolerance without insulin resistance. This mirrors the effect of fasting and very low calorie diets, which improve insulin sensitivity and reverse type 2 diabetes, but also can cause a form of glucose intolerance known as benevolent pseudo-diabetes. There is no indication that starvation (benevolent) pseudo-diabetes is detrimental. By contrast, it is associated with better health and life extension. In transplant patients, a weak association between rapamycin/everolimus use and hyperglycemia is mostly due to a drug interaction with calcineurin inhibitors. When it occurs in cancer patients, the hyperglycemia is mild and reversible. No hyperglycemic effects of rapamycin/everolimus have been detected in healthy people. For antiaging purposes, rapamycin/everolimus can be administrated intermittently (e.g., once a week) in combination with intermittent carbohydrate restriction, physical exercise, and metformin.
This may be a very, very stupid and uninformed question but it’s related to this question of glucose intolerence. If Rapamycin turns off nutrient sensing, what happens to the nutrients you ingest while this is in effect? does glucose and protien get transported the same way into cells? or do the nutrients get stored as fat? Is there something someone can point me to to explain how this works?
On days i take Rapamycin, when i’m eating I wonder what’s the point other than feeling satiated.