Is there anyone out there testing or reading up on PCSK9 inhibitors? Some trial data points to longevity gains for folks with familial hypercholesterolemia. I’ve heard Dr Attis mention them as well in some in several talks/podcasts.
PCSK9 inhibitors seem to come as monoclonal antibodies and appear to be readily available through some of the typical overseas methods.
I take Repatha. It’s helped to keep my LDL between 30 and 50 (depending on how good I’m being with diet quality) and has lowered my elevated Lp(a) to some extent. I’m not on a statin, but i do take amla, citrus bergamot and ezetimibe as well. I’ve had zero side effects from Repatha, but the shots every 2 weeks do hurt for a solid 10 seconds while medicine is being injected.
Ah, perfect. You’re exactly the kind of user I was hoping to hear from.
Did you get an Rx for it or obtain it another way?
What’s your typical cost?
Had you tried a statin before and did it have any effect on your LDL/LP(a)?
I have an Rx via my PCP. With manufacturer coupon it only costs me $15 per 12 week supply. Statins lowered my LDL, but also gave me muscle/joint/back pain and they do absolutely nothing for Lp(a) (Peter Attia has an amazing podcast involving all you ever wanted to know about Lp(a), btw). Repatha has lowered my Lp(a) about 30%, so it’s still high but I’ll take what I can get until the Lp(a)-specific drugs get through clinical trials.
I’m interested in Repatha, but I don’t think my insurance would cover it based on my numbers. Has anyone tried to source this from India? I get the usual “you must pay with Bitcoin” fraudsters, but no sign of legitimate sources. The best price on Amazon is $500/mo, which is painful, but might be worth it.
The lowest I can get my APO-B on statins is 75. Perhaps I’ll try Zetia first…
Repatha and Praluent (the 2 PCSK9 inhibitors) both have to be refrigerated, so I imagine the shipping costs from overseas might be prohibitive (and even then, could you trust that it’s been stored properly?)
I’ve been debating trying to get my doc to prescribe a PCSK9i prophylactically based on Attia’s podcasts. My ApoB is 1.12 g/L which is on the higher end of the normal range (0.59-1.25). My doc would give me a statin in a heartbeat if I asked for it, but I’ll have a more uphill climb asking for a PCSK9i.
Anyone have opinions on taking this when within normal ranges of ApoB and no FH (financial cost aside)?
I take natural, potential PCSK9 inhibitors in diet. There are a bunch of them in a traditional Okinawan diet that is associated with lowered LDL/apoB, but whether these compounds and metabolites actually inhibit PCSK9 in vivo is not demonstrated.
I think @tongMD is referring to these types of diet compounds when he says he gets potential PCSK9 inhibitors in diet:
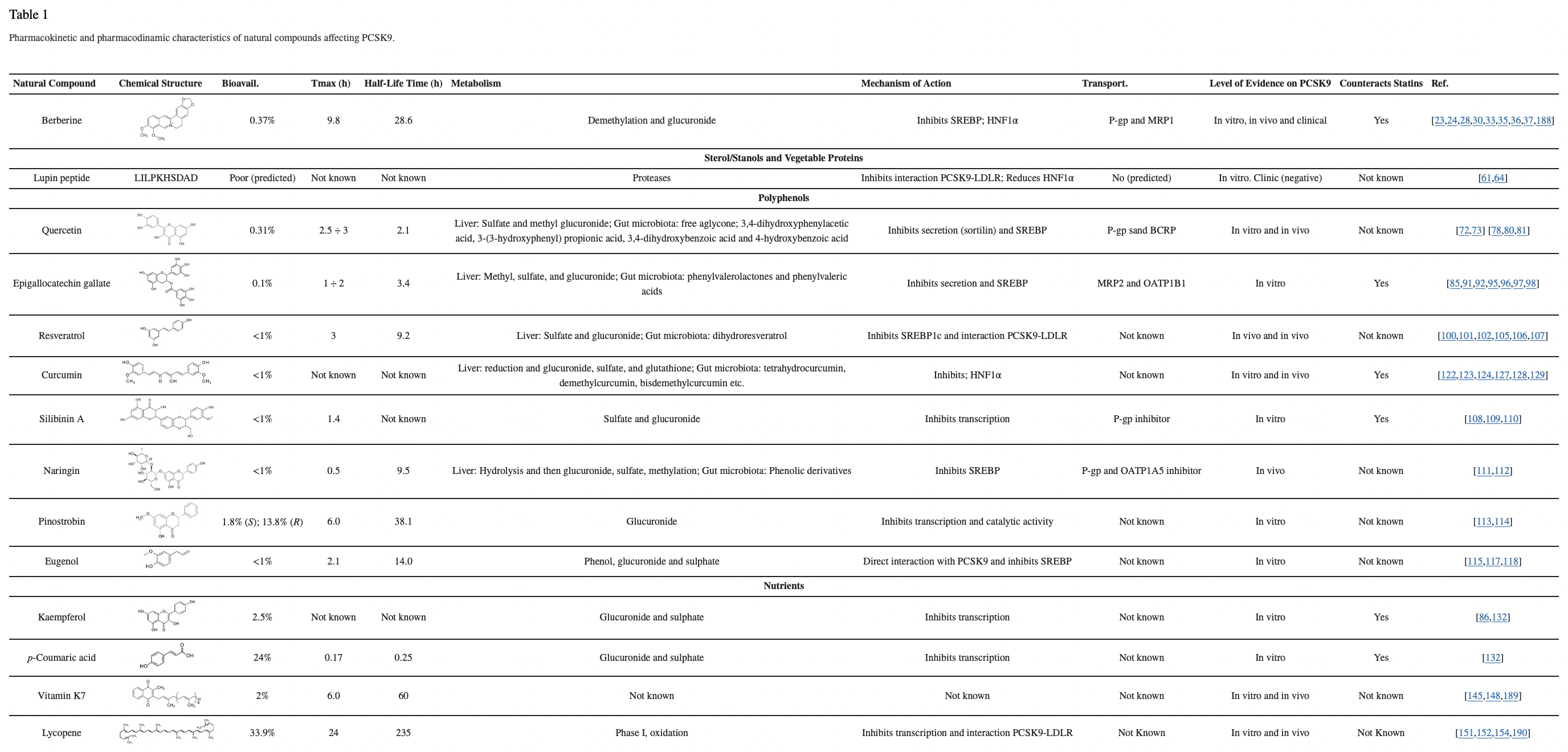
A possible breakthrough in this field may come from the discovery of new naturally occurring PCSK9 inhibitors as a starting point for the development of oral, small molecules, to be used in combination with statins in order to increase the percentage of patients reaching their LDL-cholesterol target levels. In the present review, we have summarized the current knowledge on natural compounds or extracts that have shown an inhibitory effect on PCSK9, either in experimental or clinical settings. When available, the pharmacodynamic and pharmacokinetic profiles of the listed compounds are described.
There are some other ones btw, but that’s a very nice summary. Also, one could enroll in clinical trials for editing the PCSK9 gene using gene therapy.
As for the drugs themselves, I think the benefit-to-cost ratio for most people for PCSK9 inhibitors at current prices without the indication is generally way too slim IMO. Would I consider adding it if I had say $10M+ net worth in my situation? Sure.
Oh btw, there are several natural compounds (these potential PCSK9 inhibitors) in the traditional Okinawan diet (pre-WWII, not the one that gets blindly marketed to the general public) that are P-glycoprotein/ABCB1 inducers, particularly xanthines. Some are CYP450 3A4 inducers. Then there are ones with the opposite effect that can increase rapamycin dosing (it’s not just grapefruit juice!). These are in sufficient amounts from diet alone (not concentrated food or herbal extracts) to make a big difference.
I actively avoid them carefully before the weekly rapamycin dose based on my understanding of pharmacokinetics (with consults), my own pharmacogenetics (with consults), and repeated blood tests - because they can reliably mess up my rapamycin dosing to a moderate amount.
When I use “food as medicine” as the Okinawans put it, it gets really complex really quickly with easily hundreds or more of potential compounds and metabolites with lots of possible interactions (don’t forget “gut flora as an organ” as well because these bugs make a dizzying array of metabolites and different bugs evolve or adapt - rarely see anyone mention that because it’s often unexpected), and if one is not extremely careful - it can mess with the other meds/compounds/supplements. I can only speak to how I use rapamycin - with planned crossovers and many blood tests.
The most obvious ones are tea, Okinawan sweet potato, Okinawa lime, bitter melon, and fermented soy. There are way too many foods, herbs, and spices to list as well as compounds derived from all these things. Then you have to account for cooking and preparation methods (it definitely matters big time for some of the naturally-derived compounds i.e. naturally occurring peroxidases/polyphenol oxidases, catalases, and lipoxygenases in the presence of oxygen). As well as whether you can actually source some of these different foods in the US safely or what might be suitable substitutes.
I suggest visiting Okinawa sometime with someone who can translate Okinawan and Okinawan Japanese well because there is just a lot of info out there on the internet that did not correspond with my visit to a few centenarians. I also suggest reading 1-2 original old classical texts in Chinese herbal medicine (ignore the “mystical” TCM vocabulary and pseudoscientific terms - it’s not much different than “mystical” Indian terms used in yoga that correspond to breathing and stretching practices that are suggestive for relaxation responses, lower tumor volume, and increased pain tolerance with imaging showing increased volume of the region of the brain responsible for interoception) because that heavily influenced traditional Okinawan diets. You may be surprised that they discovered natural statins and ate them well before statins were first invented.
In addition, there are also natural combinations of several alpha-glucosidase and alpha-amylase inhibitors that is very likely better than acarbose alone for long-term use such that I only use acarbose occasionally (a departure from acarbose-related lifespan literature) for convenience reasons. That’s partly why I think acarbose monotherapy might not pan out in human clinical trials if done for long enough periods of time where the effect would be less robust than this natural mix of several inhibitors that withstood the test of time (and subsequent scientific testing to verify)