You can send to me in the USA if shipping is not terribly expensive. We are having a shortage of of estrogen products and they can be difficult to come by
It would honestly be cheaper if you purchased it from where I got it. I got it from Maulik who is one of the popular sellers of Rapamycin on this website.
https://www.shreejiimpex.co.in/ is his website.
3 Likes
Thanks, I’ll do that
1 Like
At this point as a male the only estrogen related thing I am interested in trying for skin health and longevity now is 17a estradiol.
Aromatase inhibition makes me feel bad, and topical estradiol and estriol haven’t worked for obvious reasons.
2 Likes
5 Likes

https://x.com/jefftangx/status/2062225463905275973?s=20
From Gemini:
Product Identification and Source
The product shown in the image HJ5_ID5XoAEqk4d.jpeg is a customized prescription topical preparation utilizing ExoBlue™ , a specialized cosmetic compounding base manufactured by PCCA (Professional Compounding Centers of America).
Source Breakdown
-
Base Manufacturer: PCCA, headquartered in Houston, Texas. PCCA does not sell directly to consumers; instead, they supply proprietary bases and bulk chemical ingredients exclusively to licensed member compounding pharmacies.
-
Dispensing Pharmacy: The actual dispensing source is an independent compounding pharmacy, as indicated by the truncated text “…Compounding Pharmac…” printed at the top of the container label in
HJ5_ID5XoAEqk4d.jpeg. The exact identity of the retail pharmacy cannot be determined because the header text is cropped out.
Base Composition and Mechanism
ExoBlue™ (PCCA Product #30-5290) is an advanced skin-conditioning vehicle designed to optimize peptide stability and facilitate multi-pathway skin rejuvenation. Rather than functioning as an inert carrier, the base itself is formulated with a framework of active cosmetic technologies:
PCCA+ 1
| Key Ingredient | Functional Profile |
|---|---|
| GHK-Copper Peptide PURE | Stimulates fibroblast proliferation and collagen synthesis; provides the cream with its inherent light blue tint. |
| Centella asiatica-Derived Exosomes | Act as nanometric cellular messengers to accelerate natural tissue repair pathways. |
| Acetyl Hexapeptide-8 | Minimizes muscle microtensions to smooth expression lines. |
| Zinc Hydrolyzed Hyaluronate | Delivers deep trans-epidermal hydration and supports barrier integrity. |
For detailed documentation, refer to the PCCA ExoBlue™ Product Page and the official PCCA Press Release.
1 Like
Beyond Chronology: Why Your Peers See You Differently and the Real Vectors of Facial Aging
Our chronological age is a fixed metric, but our biological age is highly variable, often written directly onto the canvas of our skin. A new study published in the Journal of Dermatologic Science and Cosmetic Technology uncovers a stark divergence between the age on a person’s birth certificate and how old they actually look to an audience of their peers. By deploying a panel of over 60 non-expert, adjacent-age assessors to review standardized digital photographs of 308 Chinese women aged 15–65, researchers mapped out the precise morphological features that govern human age perception.
The overarching finding challenges common assumptions: across the entire cohort, women were perceived as an average of 1.6 years older than their actual chronological age. However, this age distortion is highly non-linear across a lifespan. Chronologically younger women bear the heaviest burden of overestimation. Strikingly, teenagers in the 15–20 age group were judged to be an average of 5.6 years older than their true age. This overestimation tapers off mid-life, stabilized between ages 41–50 where perceived age aligns closely with reality. By contrast, an inversion occurs at the oldest end of the spectrum: women aged 61–65 were perceived as an average of 2.4 years younger than their chronological baseline.
What drives these perceptual shifts? The data reveals that humanity’s internal age-estimation algorithms rely on distinct spatial and surface cues. While deep architectural structural changes like nasolabial folds and marionette lines act as global anchors for aging across all generations, superficial skin quality dictates the fine-tuning of age estimation in older adults. In youth, minor deviations from flawless skin uniformity—such as early under-eye lines or localized sagging—trigger cognitive heuristics that sharply penalize the subject, making them appear prematurely aged to observers. Conversely, older individuals who manage to maintain superior skin radiance, smoothness, and an even complexion stand out as uniquely well-preserved, driving substantial age underestimation by their peers.
Actionable Insights
For longevity practitioners and biohackers tracking appearance as a proxy for biological vitality, this study provides clear directions on where to focus therapeutic and cosmetic interventions:
-
Prioritize Mid-Face Structural Integrity Over Minor Eye Wrinkles: Marionette folds and nasolabial folds are the most heavily weighted features driving older age perception across all groups. Surprisingly, isolated markers like crow’s feet had a very low relative weight (ranking 17th out of 25 features), meaning treating them yields minor adjustments to how old you look.
-
Target Skin Tone and Glycation Deficits After Age 40: For individuals over 40, skin dullness and skin yellowness increase the risk of looking older by an effect size of 33% (Odds Ratio: 1.11–1.21) and 34% (Odds Ratio: 1.23–1.46) respectively. In the oldest cohort (61–65), skin dullness increases the odds of looking older by 68%. Interventions should focus on preventing advanced glycation end-products (AGEs) and boosting dermal microcirculation.
-
Younger Cohorts Must Prevent Mid-Face Sagging and Under-Eye Lines: For individuals aged 15–20, the presence of under-eye wrinkles increases the odds of looking older by more than two-fold (Odds Ratio: 2.38). Overall facial sagging similarly doubles the odds of appearing older (Odds Ratio: 2.04). Protecting the delicate sub-orbital extracellular matrix in early adulthood is paramount.
Source:
- Open Access Paper: An exploration study on the relationship between chronological and perceived age in Chinese women with systematic validation of a new method for perceived age determination
- Institution: Beiersdorf Innovation Center Shanghai.
- Country: China.
- Journal Name: Journal of Dermatologic Science and Cosmetic Technology.
- Impact Evaluation: The impact score of this journal is not yet officially rated or widely indexed with a standard high Impact Factor due to its recent launch in the 2024–2026 window, therefore this is a Low impact journal.
Study Design Specifications
-
Type: In vivo observational cohort study with clinical grading and cross-sectional photographic peer evaluation.
-
Subjects: 308 healthy Chinese female participants who fully completed the protocol (out of 314 originally enrolled; 6 dropped out due to personal reasons). Subjects were distributed across ten distinct 5-year chronological age intervals from 15 to 65 years old, ensuring at least 30 subjects per bracket.
Biomarker Strength: Correlation with Perceived Age
Spearman correlation coefficients (ρ) quantify the strength of the relationship between clinical structural degradation and peer-perceived age:
- Crow’s feet wrinkles: ρ=0.875 (Very Strong)
- Marionette fold severity: ρ=0.844 (Very Strong)
- Underneath eye wrinkles: ρ=0.835 (Very Strong)
- Inter-ocular wrinkles: ρ=0.824 (Very Strong)
- Middle-face cheek fold: ρ=0.819 (Very Strong)
- Upper-lip wrinkles: ρ=0.813 (Very Strong)
- Fine lines on the forehead: ρ=0.810 (Very Strong)
- Forehead wrinkles (deep): ρ=0.752 (Strong)
- Nasolabial fold depth: ρ=0.768 (Strong)
- Dropping of upper outer eyelid: ρ=0.744 (Strong)
- Glabellar wrinkles: ρ=0.662 (Moderate-Strong)
- Eye Bags: ρ=0.368 (Weak)
Critical Limitations
-
Extreme Geographical and Climatic Isolation: A major flaw is that the entire cohort was pulled from a single metropolitan region (Guangzhou, China). This restricts the findings to a population exposed to a specific high-humidity, subtropical environment. It fails to account for how alternative UV baselines, pollution variations, or diverse national skin phenotypes alter aging trajectories.
-
Subjective Scaling and Lack of Absolute Biological Clocks: The research relies entirely on visual grading atlases and subjective questionnaires. It completely lacks objective validation against hard biological aging metrics.
-
Inherent Assessor Selection Bias: Utilizing peer assessors who are actively participating in a facial appearance study introduces an observer-expectancy bias. These individuals are likely hyper-attentive to structural flaws compared to the general public, potentially inflating the recorded age overestimations.
-
Commercial Conflict of Interest: The entire study was funded, designed, and executed by personnel employed by the Beiersdorf Innovation Center Shanghai (the parent conglomerate behind major global skincare brands).
1 Like
The biggest collagen study yet reveals what actually works
A massive review of collagen research found that the supplements can improve skin elasticity and hydration while helping reduce osteoarthritis pain and stiffness.
Collagen Supplementation for Skin and Musculoskeletal Health: An Umbrella Review of Meta-Analyses on Elasticity, Hydration, and Structural Outcomes . Aesthetic Surgery Journal Open Forum , 2026; 8 DOI: 10.1093/asjof/ojag018
the following supplement was identified by Google Gemini as helpful to prevent skin aging in this query cited here: What are the best strategies to maintain your early 20s appearance for as long as possible? - #3 by RapAdmin
Google Gemini Information Summary:
Oral Polypodium Leucotomos Extract (PLE) — Evidence Summary
What It Is
Polypodium leucotomos is a tropical Central American fern whose dried leaf extract is rich in phenolic acids (caffeic, ferulic, chlorogenic, and cinnamic acids) — potent antioxidants that confer systemic photoprotection when taken orally.
Mechanisms of Action
PLE works through multiple complementary pathways relevant to skin health and longevity:
Photoprotection & UV Defense: Neutralizes UV-generated reactive oxygen species (ROS), reducing oxidative DNA damage (cyclobutane pyrimidine dimers). A landmark 1997 study in Photodermatology, Photoimmunology & Photomedicine demonstrated that oral PLE prevented acute sunburn, psoralen-induced phototoxic reactions, and — critically — depletion of Langerhans cells, the skin’s frontline immune sentinels.
Anti-Photoaging: Inhibits matrix metalloproteinase-1 (MMP-1), preserving collagen and elastin — the structural proteins degraded by chronic UV exposure and responsible for wrinkles and skin laxity. It also blocks trans-urocanic acid isomerization (an immunosuppressive UV byproduct) and UV-mediated apoptosis and necrosis.
Immunomodulation: Preserves cutaneous immune surveillance by protecting Langerhans cells, which are rapidly depleted by UV — a key mechanism behind UV-induced immune suppression and skin cancer risk.
Clinical Evidence (Level 2 — RCTs)
| Study | Design | Key Finding |
|---|---|---|
| Middelkamp-Hup et al. (2004) JAAD | RCT, n=9, skin types II–III | Oral PLE significantly reduced erythema, sunburn cells, DNA damage, and mast cell infiltration vs. placebo |
| González et al. (2017) JAAD | Human clinical study, UVB response | PLE increased minimal erythema dose (MED); 17/22 subjects showed decreased UVB-induced changes |
| Parrado et al. (2025) Nutrients | RCT, double-blind, 8 weeks | 23.8% increase in MED + 46.2% reduction in erythema intensity in treatment group |
| Choudhry (2014) | RCT, vitiligo patients | Improved repigmentation when combined with NB-UVB |
| Gonzalez et al. (1997) Photoderm | RCT | Prevented Langerhans cell depletion and psoralen phototoxicity |
A 2025 systematic review in Journal of Drugs in Dermatology (21 studies meeting criteria, 11 RCTs) concluded PLE shows “strong evidence of effectiveness” across photoprotection, photoaging, and skin cancer prevention applications.
An ongoing NIH-registered clinical trial (NCT02813902) is investigating PLE specifically for prevention of skin cancer and its precursors.
Clinical Utility for Skin Longevity
PLE is not a sunscreen replacement — it provides an SPF equivalent of roughly 3–5 — but its value is systemic: it addresses UV damage in areas topical sunscreen misses or fails (incomplete coverage, missed reapplication), and it targets the immunosuppressive and pro-aging molecular pathways that drive long-term photoaging and carcinogenesis. Typical evidence-backed dosing is 240–480 mg/day, taken before sun exposure.
Reputable Products
Heliocare — The gold standard brand, built on proprietary Fernblock® PLE technology, extensively used in clinical research. Widely available via dermatologist offices, Amazon, and pharmacies. 240 mg/capsule.
Heliocare Ultra — Higher-dose formulation (480 mg PLE equivalent) with additional antioxidants for higher-risk individuals.
Supersmart Polypodium Leucotomos Extract — 1,000 mg/day dose (500 mg per capsule); manufactured in GMP/HACCP-certified facilities; 30+ year established supplement company.
Nutricost Polypodium Leucotomos Extract — 250 mg of a 20:1 concentrate (equivalent to 5,000 mg whole leaf); NSF-certified, GMP-compliant, FDA-registered facility. Budget-accessible.
NusaPure Polypodium Leucotomos — 240 mg, 10:1 extract; cGMP-manufactured in the USA; non-GMO, vegan.
Note: Heliocare is the most clinically referenced brand by name in dermatology literature and is the product most often recommended by dermatologists specifically because its Fernblock® extract is the standardized form used in many published trials.
Sources:
- Topical or oral PLE prevents Langerhans cell depletion — PubMed (1997)
- Oral PLE decreases ultraviolet-induced damage — PubMed (2004)
- Impact of oral PLE on UVB response — PMC/JAAD (2017)
- 8-Week RCT: Red Orange + PLE on UVB skin responses (2025)
- Fernblock: Molecular Mechanisms & Photoaging Review — PMC
- Clinical Efficacy & Safety of Oral PLE — Systematic Review, SKIN Journal
- Utility of Oral PLE for Dermatologic Diseases — JDD 2025
- Oral PLE for photodermatoses, 57 patients — PubMed
- NIH Clinical Trial: PLE in Skin Cancer Prevention (NCT02813902)
- Combination oral + topical PLE vs. actinic keratosis — Wiley 2023
- Heliocare on Amazon
- Nutricost PLE
Here’s a pricing summary for each product, with direct purchase links:
| Product | Dose / Count | Approx. Price | Buy Link |
|---|---|---|---|
| Heliocare (standard) | 240mg Fernblock®, 60 caps | ~$37 retail / ~$25 with coupons | Amazon · LovelySkin |
| Heliocare Ultra | 480mg Fernblock® + vitamins C/E, lutein, lycopene, 30 caps | ~$40–$42 | Dermacare Direct · Amazon |
| SuperSmart PLE | 1,000mg (4:1 extract), 90 veg caps | ~$19 | SuperSmart Direct · Walmart · Target |
| Nutricost PLE | 250mg (20:1 extract = 5,000mg equivalent), 240 caps | ~$15–$17 | Nutricost.com · Amazon |
| NusaPure PLE | 240mg (10:1 extract = 2,400mg equivalent), 200 veg caps | ~$18–$22 | NusaPure Direct · Amazon |
Value note: Nutricost and SuperSmart offer the best cost-per-dose for budget-conscious buyers. Heliocare commands a premium as the clinically referenced brand with standardized Fernblock® extract — worth it if you want the formulation closest to what was studied in RCTs.
Sources:
2 Likes
What’s Really Causing Your Skin to Age?

What’s Really Causing Your Skin to Age?
I. Executive Summary
The core thesis presented by Dr. Hillary Lin centers on skin elasticity as an actionable, external surrogate biomarker for systemic physiological health, rather than a merely aesthetic metric. Cutaneous aging is governed by the structural integrity of the dermal extracellular matrix (ECM), specifically the interplay between elastin fibers—which function as mechanical springs providing tissue compliance and recoil—and collagen scaffolds that supply tensile strength. Chronological, intrinsic aging drives a genetically programmed decline in matrix synthesis, which is drastically compounded by extrinsic photoaging and environmental insults.
Mechanistically, cutaneous degeneration is orchestrated by four primary pillars: intrinsic senescence, elastic fiber fragmentation, persistent low-grade chronic inflammation (inflammaging), and the pathological upregulation of Matrix Metalloproteinases (MMPs). Enzymes such as MMP-1, MMP-2, and MMP-9, which normally manage physiological tissue remodeling, become hyperactive under the influence of ultraviolet (UV) radiation and oxidative stress, causing unchecked degradation of structural proteins. This destruction is further exacerbated by the accumulation of Advanced Glycation End-products (AGEs), where non-enzymatic glycation cross-links dermal proteins, rendering once-flexible fibers rigid and brittle.
To counter this cascade, a multi-modal therapeutic framework is proposed, bridging systemic lifestyle factors and targeted biomolecular interventions. At the foundational tier, regular resistance exercise emerges as a powerful systemic intervention, clinically demonstrated to suppress circulating inflammatory cytokines and expand dermal thickness via ECM gene activation. Nutritional optimization focuses on the targeted ingestion of hydrolyzed collagen peptides, which are broken down into specific bioactive dipeptides that directly stimulate dermal fibroblasts to synthesize new ECM networks while simultaneously inhibiting MMP activity. Photoprotection via broad-spectrum, daily mineral sunblock is mandatory to shield the dermis from the destructive wavelengths of both UVA and UVB light, which otherwise deplete the structural matrix. Advanced topical care integrates prescription retinoids to accelerate cell turnover and L-ascorbic acid to quench free radicals and drive collagen synthesis. Ultimately, cutaneous longevity cannot be achieved through superficial topical applications alone; it requires a coordinated, inside-out strategy that systematically addresses systemic inflammation, oxidative stress, glycation, and cellular mechanical signaling.
II. Insight Bullets
- Skin Elasticity as a Biomarker: Cutaneous elasticity serves as an external physiological proxy reflecting systemic state, directly tracking cellular hydration, nutritional competence, and endocrine balance.
- Elastin Mechanical Recoil: Elastin fibers operate as physical springs within the dermal layer, granting tissue compliance and allowing the skin to return to its baseline geometry after mechanical distortion.
- Collagen Structural Framework: Dermal collagen functions as structural scaffolding, providing the high tensile strength and rigidity required to hold cutaneous architecture in place.
- Intrinsic Degradation Vector: Programmed chronological senescence naturally dictates the gradual fragmentation, disorganization, and diminished production of both collagen and elastin fibers over time.
- Extrinsic Aging Wavelengths: External environmental inputs, primarily ultraviolet (UV) radiation, accelerate structural degradation by transforming flexible, compliant elastic networks into brittle, fragmented structures.
- The Four-Factor Matrix of Aging: Cutaneous structural failure is driven by four discrete, interconnected biological pathways: chronological senescence, elastic fiber degeneration, chronic micro-inflammation, and accelerated enzymatic cleavage.
- Dermal Fraying Analogy: Over time, the fragmentation of dermal components causes a tightly woven architectural tapestry to fray, destabilizing the structural framework and manifesting as clinical sagging and rhytids (wrinkles).
- Matrix Metalloproteinase Overactivation: Endogenous zinc-dependent endopeptidases (specifically MMP-1, MMP-2, and MMP-9) are pathologically upregulated by environmental toxins, shifting their role from controlled tissue remodeling to systematic ECM destruction.
- Maladaptive Hormetic Thresholds: Mild, acute stressors stimulate adaptive tissue resilience, but excessive or prolonged environmental insults cross a critical threshold, triggering chronic MMP activation and tissue disrepair.
- Advanced Glycation End-Products (AGEs): Non-enzymatic glycation occurs when circulating sugars covalently bond to dermal proteins and lipids, forming rigid cross-links that render soft, springy tissues stiff and non-functional.
- Cutaneous Inflammaging: Age-associated low-grade chronic inflammation upregulates systemic pro-inflammatory cytokines like interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-Alpha), which continuously fuel MMP activity.
- Oxidative Rusting: Chronic micro-inflammation increases intracellular oxidative stress, mimicking an unmitigated “rusting” process that compromises the functional integrity of dermal cells and matrices.
- Bioactive Dipeptide Pharmacokinetics: Ingested collagen cannot bypass digestion intact; instead, it must be hydrolyzed into specific bioactive dipeptides—such as proline-hydroxyproline—to enter systemic circulation and reach target tissues.
- Fibroblast Genetic Activation: Systemically absorbed collagen dipeptides bind to dermal fibroblasts, functioning as signaling ligands that directly upregulate the transcription of type I collagen and elastin genes.
- Competitive MMP Suppression: Beyond driving new protein synthesis, specific hydrolyzed collagen peptides act as regulatory inhibitors that suppress hyperactive MMP enzymes, preserving existing dermal networks.
- Whole-Food vs. Isolated Antioxidant Toxicity: Sourcing polyphenols and flavonoids from whole-food matrices is superior to synthetic isolated megadoses, mitigating the severe hypervitaminosis and accumulation risks inherent to fat-soluble vitamins.
- Omega-3 PUFA Emulsion: Long-chain omega-3 polyunsaturated fatty acids downregulate UV-induced inflammatory pathways, optimize baseline stratum corneum hydration, and visibly reduce wrinkle depth within 12 weeks.
- Linoleic Acid Nuance: Despite common anti-seed-oil rhetoric, dietary omega-6 linoleic acid is associated with superior epidermal hydration metrics and a significant reduction in age-related skin thinning.
- Carotenoid Photoprotection: Dietary carotenoids (e.g., beta-carotene, astaxanthin) accumulate directly within cutaneous tissue, actively neutralizing UV-induced reactive oxygen species (ROS) and inducing a subtle, healthy pigment glow.
- Intestinal Transport of Hyaluronic Acid: High-molecular-weight oral hyaluronic acid resists gastric degradation, crossing the intestinal epithelium via intestinal-associated lymphoid tissue to undergo systematic distribution to peripheral connective tissues.
- Resistance Training Epigenetics: Mechanical loading via resistance exercise systematically downregulates circulating pro-inflammatory markers and enhances extracellular matrix gene expression, significantly expanding dermal thickness.
- Aerobic Microvascular Perfusion: Chronic endurance exercise enhances systemic microvascular blood flow, accelerating the delivery of essential amino acids and oxygen directly to the dermal architecture while driving down oxidative stress.
- The Complete Solar Spectrum Threat: Cutaneous photoaging is driven by the entire ambient light spectrum, including UVB (epidermal DNA damage), UVA (deep dermal matrix destruction), visible blue light, and short infrared radiation.
- UVA Deep Tissue Penetration: Due to its longer wavelength, UVA radiation penetrates past the superficial epidermis into the deep dermis, where it directly severs structural collagen and elastin cross-links.
- Mineral vs. Chemical Barrier Dynamics: Inert mineral sunblocks (zinc oxide, titanium dioxide) form a passive physical shield on top of the stratum corneum, avoiding the systemic absorption, potential toxicities, and contact sensitivities linked to chemical ultraviolet filters.
- Retinoid Kinetic Turn: Topical prescription tretinoin (vitamin A derivative) drastically compresses keratinocyte differentiation cycles and cell turnover rates while downregulating collagenase activity to smooth microtopography.
- L-Ascorbic Acid Atmospheric Volatility: Topical Vitamin C is a highly unstable molecule that oxidizes instantly upon exposure to air; standard wide-mouth cosmetic jars rapidly render the active compound biologically inert.
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Backed by Level A/B Evidence)
- Daily Broad-Spectrum Photoprotection: Apply a high-quality mineral sunblock (Zinc Oxide or Titanium Dioxide base) every morning. Regular daily use reduces cumulative photoaging markers by up to 24% over a 4.5-year period, effectively halting the UV-induced degradation of the dermal matrix. Give preference to tinted or advanced formulations that leave no white cast to maximize compliance Hughes et al., 2013.
- Hydrolyzed Collagen Peptide Supplementation: Ingest 2.5 to 10 grams of hydrolyzed collagen peptides daily for a minimum uninterrupted duration of 3 months. This input delivers bioavailable dipeptides to the bloodstream, stimulating dermal fibroblasts to upregulate collagen type 1 and elastin genes while concurrently suppressing degradative MMP enzymes PubMed / Functional et al., 2023.
- Mechanical Loading (Resistance Training): Execute structured resistance exercise sessions 2 to 3 times per week. Heavy resistance training rejuvenates aging cutaneous tissue by actively reducing circulating systemic inflammatory cytokines and directly upregulating dermal extracellular matrix synthesis, leading to measured increases in dermal thickness Nishikori et al., 2023.
- Oral Hyaluronic Acid Protocol: Supplemental intake of 120 mg of oral hyaluronic acid daily for 12 weeks. High-molecular-weight formulations survive gastric processing, pass into peripheral connective tissues via intestinal lymphatic structures, and significantly increase skin hydration while decreasing microtopographical wrinkle depth PubMed / Ingestible HA Study, 2023.
- Nighttime Prescription Retinoid Kinetics: Apply a pea-sized amount of prescription-strength tretinoin to a completely clean, dry face at night, strictly avoiding the highly delicate periorbital tissue. Tretinoin downregulates internal collagenase activity and compresses the cell-turnover timeline (Source unverified in live search for specific video trial metrics; universally validated in core dermatological literature).
Experimental Tier (Level C/D Evidence with High Safety Margins)
- Atmosphere-Isolated Vitamin C Application: Apply a topical Vitamin C (L-ascorbic acid) serum immediately after morning cleansing to neutralize free radicals and serve as an essential cofactor for collagen synthesis. To prevent immediate molecular oxidation and subsequent biological inactivation, utilize only single-use amber glass vials or airtight vacuum pumps; discard any serum showing yellow/brown discoloration.
- Gut-Skin Axis Modulation: Consume daily dietary prebiotics (high-fiber plant matter) alongside fermented probiotics (kefir, unsweetened yogurt, sauerkraut) to optimize the gut microbiome, systematically suppressing systemic inflammaging cascade metrics (IL-6, TNF-Alpha).
- Topical Hygroscopic Plumping: Apply topical moisturizers containing highly concentrated humectants, specifically glycerol and hyaluronic acid, to clean skin. Hyaluronic acid mechanically binds up to 1,000 times its molecular weight in water, drawing moisture from the deep layers to temporarily plump the stratum corneum.
Red Flag Zone (Claims Debunked or Lacking Safety Data)
- Isolated Megadose Synthetic Vitamin Ingestion: Avoid high-dose synthetic multivitamin pills, particularly fat-soluble variants (A, E). Megadosing synthetic fat-soluble compounds carries severe systemic accumulation toxicity risks; extreme over-supplementation of Vitamin D can drive dangerous hypercalcemia and electrolyte derangements, occasionally resulting in cardiac ICU admission for acute heart block.
- Isolated Synthetic Beta-Carotene Megadosing: Avoid high-dose isolated synthetic beta-carotene supplements. Randomized controlled trials show that isolated beta-carotene fails to retard photoaging and drastically elevates the incidence of lung cancer in individuals with a history of smoking Hughes et al., 2013. Excess intake also triggers benign carotenemia, physically discoloring the skin to a yellow-orange hue.
- Aggressive Retinoid Application Overuse: Do not apply large volumes of tretinoin or place it on thin periorbital regions. Over-application triggers severe retinoid dermatitis (“retinol burn”), presenting as acute inflammation, barrier destruction, and peeling.
- Retinoid Application Without Sunscreen: Never implement a nighttime retinoid protocol without implementing rigorous next-morning broad-spectrum photoprotection. Retinoid cell-turnover acceleration leaves the fresh epidermal layer highly vulnerable to solar radiation, paradoxically worsening photoaging outcomes if left unprotected.
4 Likes
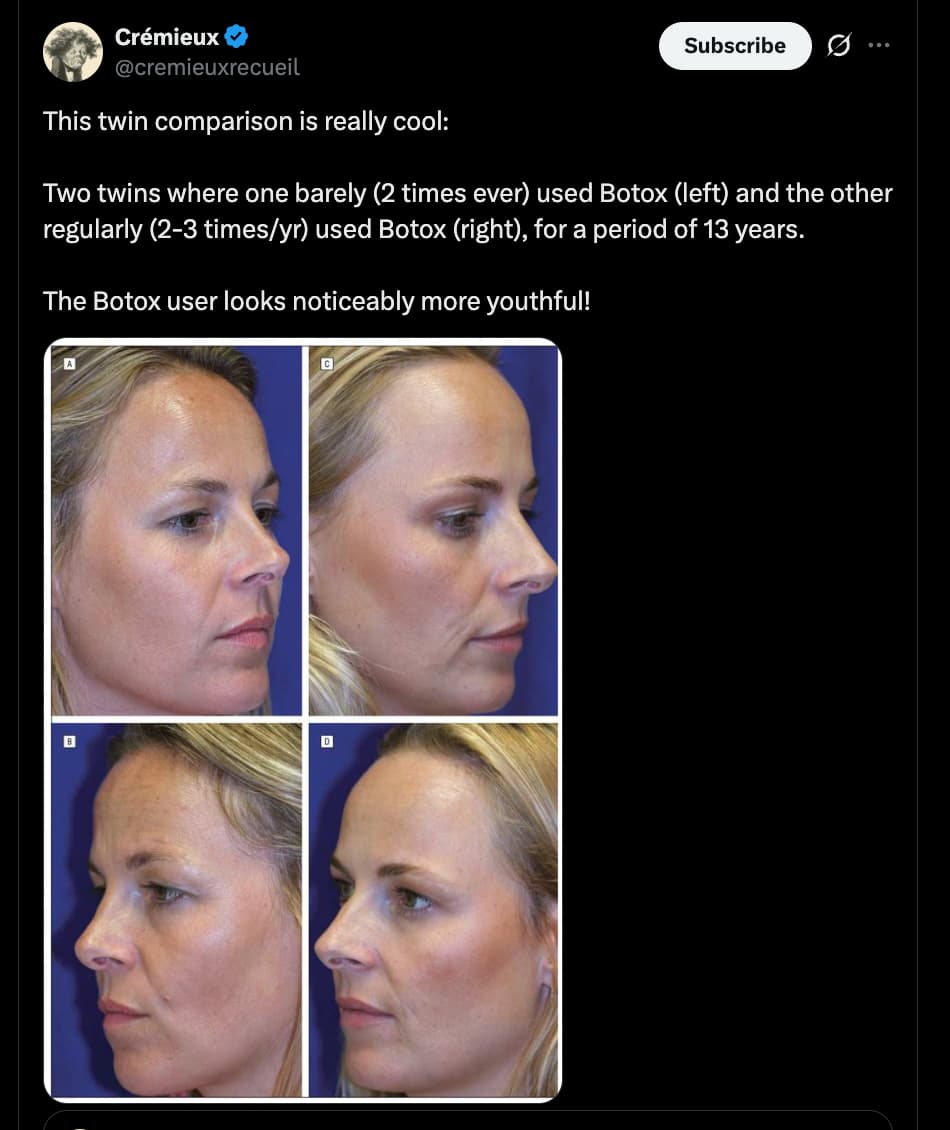
The Twin Who Froze Time: A 13-Year Botox Experiment Written on Two Identical Faces
Over 13 years, one identical twin received regular Botox to the forehead and brow while her genetically identical sister did not — and the treated twin’s deep, etched-in wrinkles simply never formed. The paper argues that long-term neuromuscular paralysis doesn’t just mask wrinkles temporarily but prevents the permanent “imprinting” of facial lines altogether.
Identical twins are the closest thing biology offers to a controlled experiment on a human face. Same genes, same collagen, same tendency to crease. So when two 38-year-old identical sisters walked into a Los Angeles clinic with dramatically different foreheads, the difference demanded an explanation — and the explanation, according to this report, was Botox.
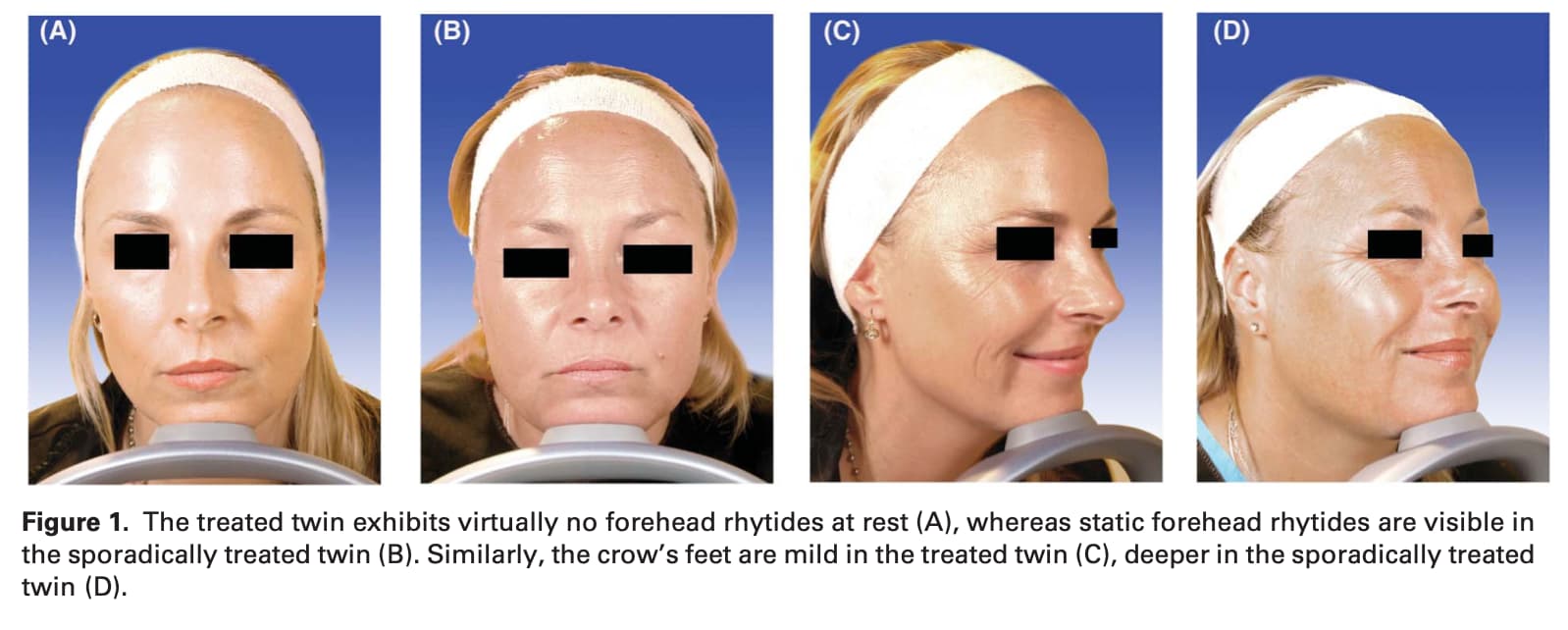
One twin had received botulinum toxin type A injections into her forehead and frown-line muscles roughly two to three times a year for thirteen years. Her sister had been injected only twice, ever. The result was visible at rest, with no expression at all: the regularly treated twin’s forehead and glabellar (“frown line”) regions were smooth, while her sister carried the fixed, etched horizontal and vertical lines that most people accumulate by midlife.
The core idea is subtle but important. Everyone knows Botox smooths wrinkles while the muscle is chemically frozen. This report argues something further — that by preventing decades of repetitive muscle folding, the skin never develops permanent creases in the first place. These so-called imprinted lines are normally one-way streets: once the dermis and epidermis break down along a fold, no amount of fresh Botox reverses them. You need fillers or laser resurfacing. The twin comparison suggests that starting early and continuing indefinitely may sidestep that damage entirely.
A useful internal control strengthens the picture. Neither twin was treated in the lower face, and both showed comparable nasolabial folds and general aging there. That the divergence appeared only in the treated muscles — and not across the whole face — argues against the simpler explanation that one sister just aged faster.
The caveats are enormous, and the paper is candid about being an observation rather than a trial. This is a single pair of twins, documented photographically, authored by a physician with a direct financial stake in the manufacturer. It proves nothing on its own. But as a proof-of-concept for the “prevention, not just correction” hypothesis, two identical faces telling opposite stories is a striking piece of visual evidence — and one that has shaped cosmetic practice ever since.
Actionable Insights
The practical takeaway is narrow but real: for the specific goal of preventing etched forehead and frown lines, sustained low-frequency treatment appears to work as prophylaxis, not merely cosmetics. The dosing that produced this outcome was modest and stable — roughly 20 to 30 units total across the forehead and 15 to 25 units in the glabella, delivered only two to three times yearly, unchanged across 13 years.
On effect size: this must be stated plainly. No quantitative effect size can be calculated from this paper. There are no measurements, scores, rating scales, or continuous variables — only side-by-side photographs. The “magnitude” is a binary qualitative judgment (lines present versus absent). Any Cohen’s d, relative risk, or hazard ratio would be fabricated. The honest real-world magnitude is: “in one twin pair, imprinted lines were categorically absent in the treated sister.” That is a case observation, not an effect size.
Two secondary practical points survive scrutiny. First, the treated twin’s clinical benefit reportedly held for at least 6 months per session without dose escalation — consistent with prior literature suggesting repeated dosing may lengthen duration. Second, crow’s feet differences appeared only on smiling, not at rest, because that region had been treated for just 2 years — implying the “prevention” effect requires long time horizons, not quick wins.
Context / Source
-
Full title: Long-Term Effects of Botulinum Toxin Type A (Botox) on Facial Lines: A Comparison in Identical Twins
Paper available on Sci-Hub Here: https://sci-hub.st/storage/2024/4123/a175a75273bbf1af4fa648dbfecda1bc/binder2006.pdf - Author / Institution: William J. Binder, MD, Department of Head and Neck Surgery, UCLA School of Medicine, Los Angeles — USA
- Journal: Archives of Facial Plastic Surgery, 2006;8:426-431 (this AMA journal later became JAMA Facial Plastic Surgery; now discontinued)
- Access: Paywalled (AMA/JAMA Network archive)
- Article type: Classified as “Surgical Technique,” but functionally a single case report / twin case study
- Impact Evaluation: The impact score of this journal is approximately 1.5, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a Low impact journal.

and another similar type of study:
Full paper:
Long-Term Effects of OnabotulinumtoxinA on Facial Lines: A 19-Year Experience of Identical Twins
3 Likes
The study followed 22 adults who underwent three treatments with Candela’s 1940 nm non-ablative fractional laser. Researchers used a split-face design, treating one side of each participant’s face while leaving the other untreated for comparison.
Instead of relying only on photographs or physician assessments, the team examined tiny molecular markers known as DNA methylation patterns. These are chemical tags that sit on DNA and help regulate how genes behave without changing the genetic code itself. Scientists increasingly use these patterns as one of the most reliable ways to estimate biological aging.
Across more than 3.8 million sites in the genome, the researchers found that the laser treatment shifted DNA methylation in the opposite direction of normal skin aging at nearly 84% of the age-related sites that responded to treatment.
Equally notable was the timeline. The molecular changes did not appear immediately after treatment. They emerged about a month after the treatment series, continued to strengthen over the following months and remained stable six months later, suggesting the skin was continuing to remodel itself well after the laser sessions had ended.
1 Like
As a life long Botox user, I’ll give my 2 cents…
The smiling pictures are meaningless because if you have Botox you’ll always have fewer wrinkles because your face won’t move as much… note, the un-Botox’d twin has cheeks that rise up naturally when she smiles which causes more eye wrinkles (not relevant but she has a much prettier smile due to this fact)
And at rest
While Botox MIGHT have prevented the fine lines, we don’t really know. The un-botox’d twin has noticeably more sun damage. She is more tanned (not necessarily relevant) but notice the sun spots on her forehead compared to the paler twin.
The un-botox’d twin has less sagging around her mouth, fwiw. Not relevant.
Hope you enjoyed my ted talk.
8 Likes
I noticed the same things!
1 Like
I hope you are sitting down because this is a EUREKA moment!!!
A couple of months ago I posted about my new pigmentation (it’s mild, but having anything was just a hmmm compared to being very clear).
I was using zinc fairly often until last fall-ish. Then I switched exclusively over to BOJ (Korean spf) because I learned that has better spf coverage than even zinc.
Well, today I spent the morning with Fable and my mind is forever blown.
I gave ‘him’ a photo and he immediately told me what kind of pigmentation I have. He said it’s nothing IPL or CO2 would address.
I told him which windows I have and he said my windows block UVB and almost all UVA, so I barely need spf at home.
So, how am I getting pigment you ask? Well, I learned that light actually causes pigmentation, and no amount of spf is going to block the light… WHAAAATTTTT???
So, my issue was never about zinc vs chemical or even wearing it at all when inside. The protection was a result of my zinc being tinted!!! It was the tint my dear Watson, the tint!!
Iron oxides are the key to blocking light, be in it makeup or tinted spf. The lack of tint is why I’m getting pigmentation while indoors (or anywhere)
He suggested if I’m home for the day, slap on tinted spf or makeup.
If going out, slap one of those on over my chemical spf. Basically, bare faced is not my friend.
I asked him to summarize for you……
Why your sunscreen isn’t stopping your pigmentation (and iron oxides are the missing piece)
SPF only grades UVB, and UVA filters cover UVA. But visible light, the light you can see, passes straight through every non-tinted sunscreen on the market, mineral or chemical. Zinc particles in modern sunscreens are sized to be cosmetically clear, which by definition means transparent to visible wavelengths.
Turns out visible light is an independent driver of pigmentation. In melasma RCTs (Boukari 2015, Dumbuya 2020), patients using sunscreen plus iron oxides pigmented significantly less than patients using the identical sunscreen without them. Visible light activates melanogenesis via opsin-3 signaling in melanocytes, and the effect is strongest in people already prone to pigment. It also generates reactive oxygen species, so it contributes to photoaging generally, not just spots.
Iron oxides (CI 77491/77492/77499, i.e., the pigments in any tint) absorb visible light. Roughly 3% was the effective dose in the studies, which in practice means a tint you can actually see on
And no, Opus never told me this, even though it was discussed at length.
4 Likes
Thank you Beth. I sent this to my daughter who has started having pigment issues over the last few years. She lives in West Texas where it’s very hot and sunny. We have both gotten more serious about sunscreen but had no idea about the importance of it being tinted. Fortunately I normally wear makeup over my sunscreen but my daughter does not. This is invaluable information!
1 Like
Aw man I’ve resisted wearing sunscreen indoors forever.
Does this apply to red light therapy devices?
I have seen concerning pigmentation anecdotes from people using blue lights on their light therapy masks.
2 Likes
This is why physically blocking light (a hat with a brim) is better than any sunscreen (tinted or not), although you’ll still get some reflected light especially if out on the water.
1 Like
How to Stay Young With the Skin of the Dead
South Korea’s latest beauty fix is made from cadaver skin
Sara Yoon recalls the moment her Seoul dermatologist described the clinic’s newest offering. His English wasn’t perfect, making the pitch sound even more like science fiction than skin care.
“It’s made from dead people,” he said.
The 40-year-old influencer and mother of two from New Jersey, who moved to Seoul in 2023, paused — but only for a moment. In the gleaming clinics of the city’s affluent Gangnam district, the treatment derived from donated human tissue has become a must-have beauty fix. Patients line up. Vials sell out. Shares of L&C Bio Co., the small Korean biotech company leading the boom with its Re2O skin booster, have more than doubled over the past year.
Yoon’s fleeting hesitation reflects just how quickly one of modern medicine’s most unlikely ingredients has entered South Korea’s beauty mainstream, where the pursuit of dong-an — “youthful face” — fuels a constant search for the next breakthrough treatment. But the boom is also drawing regulatory scrutiny. Critics question the ethics of using donated human tissue in cosmetic procedures and whether growing demand could divert supplies from traditional medical uses such as breast reconstruction and burn treatment.
The Re2O treatment involves injecting a 6-milliliter vial of extracellular matrix, or ECM, derived from processed human skin directly into a patient’s face and neck. (“Layer skin over skin,” reads the tagline.) It provides an immediate dermal scaffold that fills fine lines, tightens pores and creates a structure into which the body’s own cells can grow. Dermatologists charge 600,000 won to 800,000 won ($400 to $530) per session, compared with 200,000 won to 300,000 won for conventional skin boosters.
The skin used in Re20 comes from tissue donated in the US and certified by the Washington-based Association for Advancing Tissue and Biologics, which sets standards for the safe use of donated human tissue and the donor authorization process. A few other Korean companies, including Hans Biomed Corp. and CG Bio Co., also make skin boosters derived from AATB-certified human tissue.
Read the full story: Human Skin Is the Newest Ingredient in the K-Beauty Boom
1 Like
Currently experimenting with a home made melatonin face serum.
Why I like it more than retinoids:
Retinoids on paper are great. In practice I find they irritate me to no end. I’m not sure I’ll ever be able to use them on my face which is unfortunate. No matter how strict I am with sunscreen I always end up with red skin. I’m just too prone to it.
But I am a very enthusiastic person. I do think I tend to use a new thing too much. In the future I will try strictly experimenting with a low % adapalene 2-3x a week.
Melatonin on the other hand no only can be put on in the morning in the sun, it shows photoprotective effects in studies. This is a huge bonus. It is currently my only major skin active AM and PM.
My home made recipe is very cheap as well, not that retinoids are expensive if you get them from Indian pharmacies.
My recipe:
I put pure melatonin powder in a glass jar with propylene glycol. I submerged the bottom part of the jar in warm/hot water and stirred continually to dissolve it into solution. Once dissolved I would add more and continue this process until it stopped fully dissolving. Once I reached this stage I then took my usual moisturizer, Cerave PM, and started adding this in and stirring it to incorporate.
In hindsight I think having the moisturizer in a container and slowly adding the melatonin solution and mixing it in would be a better method as the way I did it resulted in the moisturizer clumping up and being hard to fully mix in. Eventually it did mix in, I just resubmerged the bottom of the jar in warm/hot water and stirred vigorously.
I find this melatonin serum to be perhaps a little too concentrated. If I put it on and don’t put moisturizer on top right away it feels like it burns a bit. But this might be the propylene glycol.
Things to consider:
- From what I can see you need to keep this in the refrigerator. This is the only flaw for me. I’d rather keep it in the bathroom with my moisturizer for more streamlined use. Perhaps decanting a small amount into a small amber glass jar is viable.
- If you want to get a specific melatonin % in your serum you will need strict measurement. I’m not sure what the saturation point of melatonin in propylene glycol is, but 12.5% in studies was what was needed for maximum photoprotection. Lower % is useful for other anti-aging effects.
- My thought was to just get the highest % and get all of the benefits, especially since bulk melatonin powder isn’t really that expensive. Especially compared to buying premade melatonin serums.
I had Claude AI summarize all of the major studies on topical melatonin:
“Clinical Studies Using Topical Melatonin” (2024) — reviews 18 clinical trials on topical melatonin for photoprotection, anti-aging, and hair growth (PubMed search through Dec 2023).
“Unveiling the Anti-Aging Potential of Topical Melatonin: A Systematic Review” (2026) — broader pooled analysis. Topical melatonin (alone or combined) associated with skin hydration up to +59.5%, firmness up to +30%, wrinkle depth reduction −11% to −31%. Mechanistic findings: downregulated mTORC1, decreased MMP-1, increased collagen 17A1, fibrillin-1, and mitochondrial markers (TFAM, MTCO-1, VDAC).
UV protection / erythema
- Bangha et al., dose-response (1996) — 20 volunteers, UVB exposure on lower back, 0.05%/0.1%/0.5% melatonin gel vs. carrier alone. Clear dose-response; 0.5% performed best, significant at 8h post-irradiation. Suppression of UV-induced erythema by topical treatment with melatonin (N-acetyl-5-methoxytryptamine). A dose response study - PubMed
- Bangha et al., timing study (1997) — melatonin gel applied 15 min before vs. 30/240 min after UV exposure. Pre-exposure application almost completely suppressed erythema; post-exposure application showed no protective effect. This is the key timing data point. Suppression of UV-induced erythema by topical treatment with melatonin (N-acetyl-5-methoxytryptamine). Influence of the application time point - PubMed
- Dreher, Gabard, Schwindt & Maibach (1998), British Journal of Dermatology — melatonin tested alone and combined with vitamin C/E, applied 30 min pre-UV, 12 subjects (Fitzpatrick II/III). Modest protective effect from vitamins, assessed via chromametry, dermal blood flow, TEWL, and capacitance. https://academic.oup.com/bjd/article-abstract/139/2/332/6683592
- Systematic review (2017) — confirms the pattern across the pre-exposure UV literature: protective effect only when applied before exposure, most pronounced in “strong reactor” subgroups. Melatonin for prevention of erythema and oxidative stress in response to ultraviolet radiation - PubMed
Radiation dermatitis (cancer patients)
- Ben-David, Elkayam, Gelernter & Pfeffer (2016), Israel Medical Association Journal — 47 women post-lumpectomy, randomized to melatonin emulsion (26) or placebo (21), twice daily during whole-breast radiotherapy. Dermatitis occurred in 59% of the melatonin group vs. 90% of placebo. Melatonin for Prevention of Breast Radiation Dermatitis: A Phase II, Prospective, Double-Blind Randomized Trial - PubMed
- Zetner et al. (2023), Journal of Pineal Research — MELADERM trial — a larger, more rigorous double-blind RCT (48 evaluable patients, 25mg/g melatonin + DMSO cream) designed specifically to confirm the 2016 result. Primary outcomes showed no significant difference on RTOG dermatitis scores (p=0.441) or photographic erythema analysis (p=0.890) at the 2-week primary endpoint. https://onlinelibrary.wiley.com/doi/10.1111/jpi.12873
Worth flagging in your post: this is a case where the positive finding didn’t replicate in a better-powered follow-up. Good instinct to know both sides here rather than just citing the 2016 result.
Anti-aging / wrinkles
- Morganti et al. (combined oral + topical melatonin, vitamin E, beta-glucan) — showed benefit at a very low topical concentration (0.0002%), which the review authors flag as notable given how low that dose is relative to other trials.
- Sagan et al. — a higher topical concentration (0.012% alone, no added actives) was found less effective than oral melatonin (2.5mg/day) — the opposite pattern from Morganti, suggesting the co-actives (not melatonin alone) may be doing a lot of the work in these combination formulas.
- Melatosphere™ trial (2018), Cosmetics — open, evaluator-blinded, 2-month trial using a lipid-based delivery system for melatonin. 3D imaging (ANTERA 3D) showed −31% coarse wrinkle volume, −18% fine wrinkle volume, −17% melanin content. No placebo arm. https://www.mdpi.com/2079-9284/5/4/60
- “In & Out” randomized trial (2024/2025) — compared topical-only vs. topical+oral melatonin (with hyaluronic acid and apigenin) over 84 days. Combined regimen beat topical alone: hydration +23.6% vs +18.3%, wrinkle depth −18.5% vs −9.4% (p<0.05). Lipidomic analysis showed increased ceramides and triglycerides, relevant to barrier function. Lipidomic and Instrumental Evaluation of a Melatonin-Based In & Out Strategy Versus Topical Treatment in Skin Aging: A Randomized Prospective Trial - PMC and https://www.mdpi.com/2310-2861/11/11/860
Mechanism (relevant to formulation logic)
Across the review literature, melatonin’s proposed skin mechanisms are: direct free-radical scavenging, upregulation of endogenous antioxidant enzymes (SOD, glutathione peroxidase), immune modulation relevant to inflammation/dermatitis, mitophagy activation supporting mitochondrial turnover, and downregulation of mTORC1/MMP-1 with upregulation of collagen-supportive markers.
What this means for concentration/formulation choices
Pulling from the review’s concentration data across studies: 0.01% has established human skin penetration data; 0.1% has the clearest direct anti-aging trial data; photoprotection studies span 0.5% up to 12.5%; and 2.5% has the strongest overall clinical evidence base. Combination formulas (with vitamin E, beta-glucan, hyaluronic acid, or apigenin) consistently outperform melatonin alone in the anti-aging trials, so if your serum includes complementary actives, that’s consistent with where the strongest data sits.
3 Likes