A good article on where we are as far as Biological Aging Clocks right now. Christin Glorioso is the founder of the San Francisco Longevity Group (now Longevity Global), and other startups, etc.
Scientists are quantifying your biological age and testing what you can do to age more slowly or even reverse your biological age. Levels of RNA, modifications to proteins, and epigenetics change precisely within your cells with age. Where you are in terms of those changes compared to the average person your age can reveal your biological age. This is important for determining which lifestyle interventions or drugs might be able to slow down or reverse aging without having to wait for people to kick the bucket to know what worked. A one-man experiment run by wealthy tech entrepreneur, Bryan Johnson, has recently gotten a lot of press. He is using aging clocks to quantify his health and try and reduce his biological age. He claims that he has reduced his biological age by 5.1 years and that this is a world record. It’s not in fact a world record, as pointed out by Nikolina Lauc, CEO of GlycanAge, on Twitter- many of their own employees have reduced their bio age by more than this.
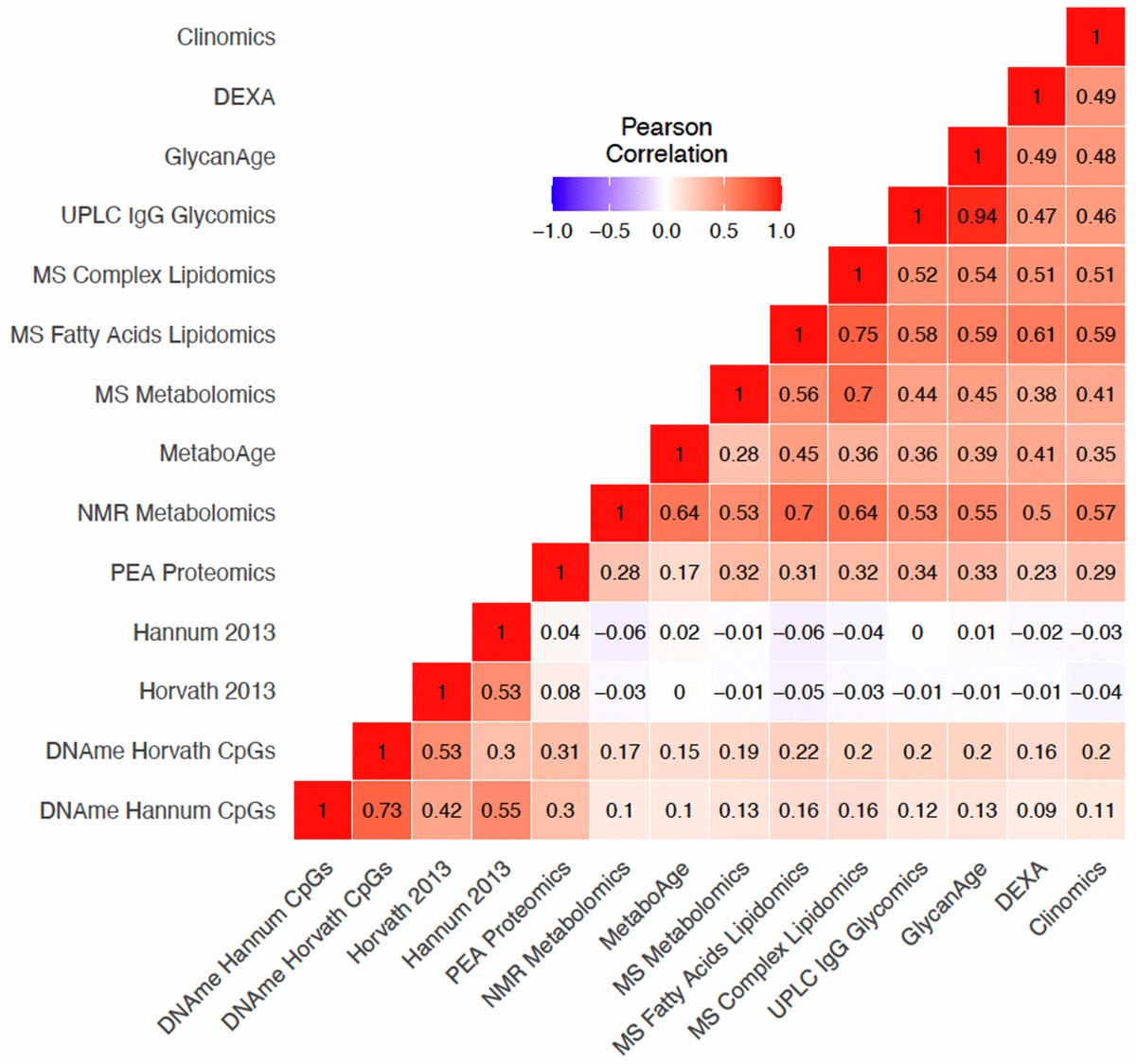
The chart that cross references the clocks is a great illustration. These can be great tools, but we should be careful not to take the number that any one test give us too literally.
That said, if your numbers are improving across multiple tests, that’s a pretty great sign that you’re doing the right thing.
30+ plants per week intake are also correlated with positive effects which may be microbiota related and probably “anti-inflammatory” to some extent.
What is Engerer offering that is new and meaningful?
He seems to have a background in solar energy for his PhD and his recent shift to “longevity space” and relationship with DoNotAge is in a marketing capacity - hence I’m not particularly optimistic on how much context he has.
There is, however, a difference between different tests producing different results and the same test producing different results (from samples taken at the same time).
My own hypothesis about aging which results from a combination of senescent cells and cellular efficiency (mitochondrial efficiency) can be in part measured by CRP. I don’t know how to measure a mixture of the mitochondrial copy number and the individual efficiency of mitochondria P/O or ATP/O, but in any event this will vary from cell to cell.
True - but at some level these commercially-sold biological and epigenetic clocks are being sold as “biological age clocks” and the public (layman) doesn’t get into the technical details and differences of the algorithms of each clock.
If your phone clock had a time that was different from your timex watch, which was different from the rolex watch time… consumers are not going to be very confident in this concept of “time” that you are promoting.
Its an issue. The research community and commercial community need to coalesce around one clock (or at most a few specific organ-related clocks), I would think.
AgingDoc brings up an interesting issue in his second tweet above.
Rapamycin has been validated dozens of times working in mice for lifespan, but none of the bio / epi clocks have been validated with any animal models or humans in terms of mapping to actual lifespans. If your bioclock is going in the wrong direction while you are on rapamycin what should you follow?
AgingDoc suggested he trusts the rapamycin research more.
Your thoughts everyone ?
@tongMD and the other docs what is your take on this issue?
I don’t use aging clocks to determine anything until they have more validation. Not to mention, commercial ones that are DTC aren’t necessarily equivalent to the one in research.
Chasing measurements and biomarkers don’t necessarily yield results until the biomarker is validated for the indicated purpose.
We previously described a DNA methylation (DNAm) based biomarker of human mortality risk DNAm GrimAge. Here we describe version 2 of GrimAge (trained on individuals aged between 40 and 92) which leverages two new DNAm based estimators of (log transformed) plasma proteins: high sensitivity C-reactive protein (logCRP) and hemoglobin A1C (logA1C). We evaluate GrimAge2 in 13,399 blood samples across nine study cohorts. After adjustment for age and sex, GrimAge2 outperforms GrimAge in predicting mortality across multiple racial/ethnic groups (meta P=3.6x10-167 versus P=2.6x10-144) and in terms of associations with age related conditions such as coronary heart disease, lung function measurement FEV1 (correlation= -0.31, P=1.1x10-136), computed tomography based measurements of fatty liver disease. We present evidence that GrimAge version 2 also applies to younger individuals and to saliva samples where it tracks markers of metabolic syndrome.
DNAm logCRP is positively correlated with morbidity count (P=1.3x10-54). DNAm logA1C is highly associated with type 2 diabetes (P=5.8x10-155). DNAm PAI-1 outperforms the other age-adjusted DNAm biomarkers including GrimAge2 in correlating with triglyceride (cor=0.34, P=9.6x10-267) and visceral fat (cor=0.41, P=4.7x10-41).
Overall, we demonstrate that GrimAge version 2 is an attractive epigenetic biomarker of human mortality and morbidity risk.
Decided to play around with the aging.ai clock. While taking Rapa and an SGLT2 my age was 48. Without those two supplements my labs indicate age of 42. I attribute this to effects on lipids. I will soon check it again after adding a statin. This is just for fun as I currently have almost no faith in these clocks.
Steven Horvath summarizes his views on the commercially available biological clocks (Queued up to his response to a question about the value of these clocks):
Well, that was unexpected. His rationale for not doing the methylation tests now is odd. Clearly there are many things a person can do. I thought the problem was the methylation clock results didn’t mean anything (or enough) for a single person.
I don’t think that we’d be on this forum if we didn’t believe that. And if the commercially available biological clocks aren’t really effective measures of the results of our experimental interventions, what are the best ways to monitor progress? Certainly blood tests, like the Levine Phenotypic Age calculations and aging.ai but those use minimal (10?) datapoints. Certainly more comprehensive measures, blood pressure, heart rate variation, ApoB, Cystatin C, A1c, testosterone, etc,etc, should give a more accurate picture (and exactly what many of us measure). What would be handy is a chart showing how different interventions influence the different markers - some are obvious, of course, statins and lipids but some aren’t. Astaxanthin for example, what markers would you expect to change?
I’m trying to optimize my biomarkers the best I can before starting rapamycin and then see if just adding rapamycin improves those markers further. Just need to settle on what markers give the best picture to measure progress and be sure I include them.
From reading here, I see that the Levine Phenotypic Age for some people got worse after starting rapamycin.