Also a note of caution: Tenofovir impairs enzyme that stops cells ageing | aidsmap
1 Like
Measured biological markers that showed improvements:
- IL-6 (decrease)
- hs-crp (decrease)
- A1c (decrease)
- Naive CD4+ Tcells (increase)
- Regulatory T cells (increase)
- neutrophils (decrease)
6 Likes
Curious how this might compare to maraviroc. This is data from humans vs maraviroc data for brain and muscle health from mice.
2 Likes
I’ve never heard of this drug, so wanted to understand how it is typically used, how long it’s been used, and by how many people it has been used by. So, basically, how much do we really know about the drug and how much experience do the medical professionals have with the drug. Here is the result I got. Basically it’s been on the market for about a decade, it’s typically used on a daily basis by millions of people, on an ongoing basis (likely for years). Side effect profile seems pretty benign.
Descovy (emtricitabine 200 mg / tenofovir alafenamide 25 mg) is a nucleoside reverse transcriptase inhibitor (NRTI) fixed-dose combination. It serves as a “backbone” for antiretroviral therapy (ART) and a primary option for Pre-Exposure Prophylaxis (PrEP).
FDA Approval History
Descovy’s approval history is defined by its transition from an HIV treatment component to a preventative blockbuster.
- April 4, 2016: Initial FDA approval for the treatment of HIV-1 infection in adults and pediatric patients (12 years and older, weighing ≥ 35 kg), to be used in combination with other antiretroviral agents.
- September 2017: Expanded indication for HIV-1 treatment to include pediatric patients weighing between 25 kg and 35 kg.
- October 3, 2019: FDA approval for Pre-Exposure Prophylaxis (PrEP) . This was indicated for at-risk adults and adolescents (≥ 35 kg) to reduce the risk of sexually acquired HIV-1, with a specific exclusion for those at risk from receptive vaginal sex due to lack of clinical data in that population at the time.
- January 2021: Further expansion of pediatric treatment indications to include children weighing at least 14 kg to <25 kg (using a lower-strength 120 mg/15 mg tablet).
Typical Prescription Practices
Descovy is favored in clinical practice over its predecessor, Truvada (TDF/FTC), due to its improved safety profile regarding bone mineral density and renal function.
1. Dosage and Administration
- Standard Adult/Adolescent Dose: One tablet (200 mg emtricitabine / 25 mg TAF) taken orally once daily , with or without food.
- HIV Treatment: Must be used as part of a complete regimen (e.g., with an integrase inhibitor like dolutegravir). It is not a standalone treatment for HIV.
- PrEP: Taken as a standalone daily pill.
2. Clinical Requirements & Duration
- Renal Monitoring: Not recommended for patients with an estimated creatinine clearance (CrCl) below 30 mL/min .
- HIV Testing (PrEP): Prescribers must confirm a negative HIV-1 status immediately before initiation and at least every 3 months during use.
-
Duration: * Treatment: Lifelong, as HIV is a chronic managed condition.
- PrEP: Continued as long as the individual remains at high risk for HIV acquisition.
Estimated Number of People Treated
As of early 2026, Descovy remains one of the most widely prescribed HIV medications globally, particularly in high-income markets.
| Category | Estimated Patient Count (Approx. 2025-2026) | Source/Context |
|---|---|---|
| U.S. PrEP Users | ~270,000 – 300,000 | Based on ~600,000 total PrEP users in the US with Descovy holding a ~45% market share. |
| U.S. HIV Treatment | ~300,000 – 400,000 | Gilead’s TAF-based regimens hold >52% of the US HIV treatment market. |
| Global Reach | Millions (Cumulative) | Gilead reports that over 10 million people in low-to-middle-income countries use their HIV therapies; Descovy is a primary component of these regimens globally. |
2 Likes
Side Effect Profile and Incidence
The following table summarizes the incidence of adverse reactions reported in the pivotal DISCOVER trial (PrEP) and broader HIV-1 treatment studies.
| Adverse Reaction | Frequency (Incidence) | Clinical Context |
|---|---|---|
| Nausea | 4% – 10% | Most common “startup” symptom; occurs in early treatment weeks. |
| Diarrhea | 5% | Generally mild and transient. |
| Headache | 2% | Often associated with the initiation phase. |
| Fatigue | 2% | Reported primarily in PrEP populations. |
| Abdominal Pain | 2% | Includes upper abdominal discomfort. |
| Weight Gain | Variable | TAF is associated with a mean gain of 1–2 kg more than TDF over 48–96 weeks. |
| Lipid Elevations | Significant | Increases in total cholesterol, LDL, and triglycerides (vs. TDF). |
Resolution and Duration
Most common side effects are categorized as “startup” symptoms.
- Timeline: Symptoms like nausea, headache, and gastrointestinal distress typically manifest within the first 1 to 4 weeks of therapy.
- Resolution: For the vast majority of patients, these side effects resolve spontaneously as the body adapts to the medication. Clinical guidelines often recommend “weathering” the first month before considering a switch, as symptoms rarely persist beyond the initial phase.
- Permanent Effects: Metabolic changes (weight and lipids) and bone/renal markers are persistent throughout treatment and do not “resolve” over time while the drug is continued.
Discontinuation Rates in Clinical Studies
Descovy demonstrates exceptionally high retention rates in controlled environments.
- DISCOVER Trial (PrEP): Only 1% of participants discontinued Descovy due to adverse events (AEs) over a 96-week period, compared to 2% for Truvada.
3 Likes
I find this intervention very interesting and compelling because it seems low risk (older, well-used drug with millions of users who use it for years at a time, mild side effect profile, low cost, easily purchased) and with some very measurable endpoints that we can individually monitor.
The biggest risk is probably if someone (friend, significant other or family member) sees the drug in your medicine cabinet and suddenly thinks you’re HIV+…
What is especially interesting to me is that we can very easily replicate the essence of this study ourselves by simply taking the drug, measuring our biomarkers (many of us here already use PhenoAge on a regular basis, as well as some of the other BioAge clocks), so can very quickly validate the results in a broader population cohort, share our data here, and move the science forward.
I really liked @argonaut 's AI analysis of the “fit” of this drug to his specific situation. That seems like a good analysis that everyone can relate to.
For me, the biggest issue is the potential for drug-drug interactions, or drug-supplement interactions, that I may run into. Because of this concern, I developed this prompt that I devised (see the full prompt posted in the “Prompts” thread here: Using AI for Health and Longevity and Research - Your Favorite Prompts - #144 by RapAdmin
Given the results of this prompt (see below) I can see that I’d likely want to pause a few supplements like curcumin, perhaps pause empagliflozin, perhaps pause rapamycin for a month or more, and do monthly blood testing to track renal function.
Mechanistic Conflict & PD Analysis
Transporter Competition (P-gp and BCRP)
TAF is a substrate of P-glycoprotein (P-gp) and Breast Cancer Resistance Protein (BCRP). Several compounds in your stack, most notably Curcumin (Meriva) and Rapamycin, are known inhibitors or substrates of these transporters. Curcumin significantly inhibits P-gp and BCRP in vitro, which may increase the systemic bioavailability of TAF, potentially increasing the risk of dose-dependent toxicities.
Renal Clearance Bottleneck
While TAF is significantly less nephrotoxic than its predecessor (TDF), it still requires renal monitoring. Your stack includes Empagliflozin (SGLT2i), Bempadoic Acid (which can increase serum creatinine by inhibiting OAT2), and Pravastatin. The cumulative burden on renal tubular secretory pathways (OAT1/3, OCT2) creates a theoretical bottleneck.
PD Conflict: Mitochondrial Health vs. NRTI Mechanism
A significant geroscience conflict exists here. Nucleoside Reverse Transcriptase Inhibitors (NRTIs) like FTC and TAF are known to inhibit DNA polymerase-gamma (Polγ), the enzyme responsible for mitochondrial DNA (mtDNA) replication.
- Effect: This can lead to mtDNA depletion and mitochondrial dysfunction.
- Longevity Antagonism: Your use of Rapamycin and Empagliflozin aims to optimize mitochondrial mitophagy and metabolic efficiency. Chronic NRTI use may partially negate these benefits by inducing subclinical mitochondrial stress.
3. Risk Stratification Table
| Interaction Pair | Risk Level | Mechanism | Potential Clinical Outcome | Recommended Action |
|---|---|---|---|---|
| TAF + Curcumin (Meriva) | Medium | P-gp and BCRP inhibition by Curcumin increases TAF absorption. | Increased systemic TAF exposure; potential for increased renal/bone toxicity. | Monitor Cystatin-C and serum creatinine. Consider spacing doses. |
| FTC/TAF + Empagliflozin | Medium | Additive renal hemodynamic changes and competition for tubular secretion. | Potential decline in eGFR; altered drug clearance. | Baseline and quarterly BMP; monitor for glycosuria changes. |
| TAF + Rapamycin | Medium | Both are P-gp substrates; potential for competitive inhibition. | Unpredictable fluctuations in Rapamycin trough levels. | If Rapamycin is used for longevity (weekly), ensure TAF is stable; monitor Rapamycin levels. |
| Bempadoic Acid + FTC/TAF | Medium | Bempadoic acid inhibits OAT2; potential minor competition with TFV (OAT1/3). | Elevation in serum creatinine, masking actual changes in eGFR. | Use Cystatin-C instead of Creatinine for more accurate GFR tracking. |
| NRTI Mechanism + Longevity Stack | Medium | Inhibition of Polγ vs. mTOR/SGLT2-mediated mitogenesis. | Antagonism of mitochondrial optimization goals. | Monitor biomarkers of mitochondrial health (Lactate/Pyruvate ratio). |
3 Likes
Is Truvada looking promising for the aging markers?
Seems quite safe from your posts about it.
2 Likes
It didn’t seem effective (and has more renal problems than Descovy) in this study.
3 Likes
This is probably a top 5-10 longevity drug as of right now. The population of the study is actually humans, that are free of diseases, and are relatively young. The markers that this claim to improve can be measured by laymen at any decent lab, and results can be seen in under 6 months. Very few longevity drug candidates fit that criteria. Interestingly to me, improvements were made even in this relatively young population.
6 Likes
I agree. Not only where these gains made in a young population, they were very significant gains. I would think it would be harder to move the needle in a young healthy group.
4 Likes
Seems like we’d hear about it somehow if AIDS patients taking the drug were getting younger.
2 Likes
Anyone who decides to take an HIV drug for anti aging better hide the bottle whenever a woman (or man) comes over. Imagine having to explain that one ![]()
8 Likes
They are living a lot longer it seems (even longer than we straight males).
But, It’s probably extremely difficult to parse out the data to distinguish between people living longer because they are HIV positive but not getting full blown AIDs (due to all the different drugs that have come on the market), vs. taking the drug prophetically, vs. other confounding factors…
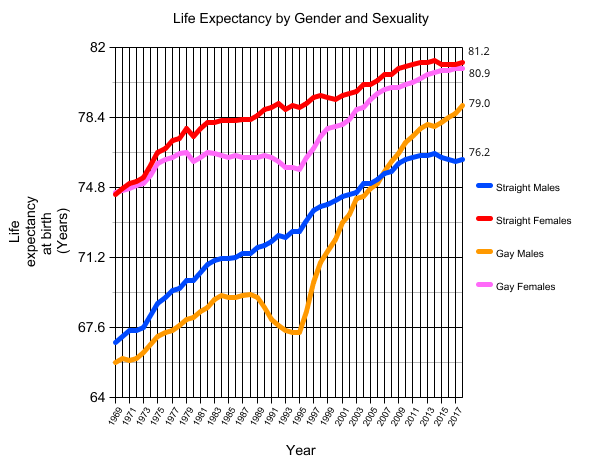
5 Likes
Striking chart. Straight up from 1995. That must be when HIV drugs came on the market.
4 Likes
Of course, the biggest issue with this paper is that we don’t see any functional measures and benefits.
So - I thought I’d dig deeper into this paper and related evidence:
Prompt:
Given the mechanisms of actions highlighted in this paper for FTC/TAF (Descovy), what would be any potential, hypothetical functional benefits that might be seen in humans given the significant reductions in biological aging clocks?
Google Gemini 3 Pro / Thinking Mode:
Based on the mechanisms of action and the system-specific biological aging clock reductions identified in the Anderson et al. (2026) paper, the following hypothetical functional benefits can be extrapolated. These benefits are centered on the suppression of the retrotransposon-inflammation axis and the subsequent reduction in systemic inflammatory tone .
1. Restoration of Immunological Resilience
The study observed a significant shift in immune cell composition, specifically an increase in the proportion of naive CD4+ T cells and regulatory T cells (Tregs), alongside a decrease in neutrophils .
-
Hypothetical Benefit: In older populations, the depletion of the naive T-cell pool is a primary driver of immune senescence, leading to poor vaccine responses and increased susceptibility to novel pathogens . A pharmacological intervention that restores these pools could theoretically enhance immunological “youthfulness” and defense capabilities.
-
Inflammatory Control: The increase in Tregs combined with reduced neutrophils suggests a shift toward a more immunoregulatory and less pro-inflammatory environment . This may reduce the chronic “bystander” tissue damage caused by hyper-active innate immune responses.
2. Neuroprotection and Cognitive Maintenance
The analysis demonstrated a significant reduction in Systems Brain Age (-2.18 years, p=0.039).
-
Hypothetical Benefit: Broader research into reverse transcriptase inhibitors (like 3TC) has shown protection against age-related cognitive dysfunction in animal models by suppressing brain-specific inflammatory signatures .
-
Mechanism: In humans, suppressing LINE-1-triggered type I interferon signaling in the central nervous system could mitigate neuroinflammation, which is a proximal driver of neurodegenerative decline and cognitive impairment .
3. Cardiovascular and Metabolic Optimization
The FTC/TAF group showed robust reductions in Systems Heart Age (-3.23 years, p=0.009) and Systems Metabolic Age (-3.38 years, p=0.005) .
- Hypothetical Benefit: These epigenetic shifts may correlate with improved arterial function and enhanced metabolic flexibility.
- Inflammatory Proxies: The study identified a significant reduction in DNAm-derived IL-6 levels . Because IL-6 is a key driver of atherosclerotic plaque progression and insulin resistance, suppressing its signaling through retrotransposon inhibition could theoretically delay the onset of cardiovascular disease and metabolic syndrome .
4. Slowing the Pace of Biological Decay
The DunedinPACE clock, which measures the “speed” of aging, showed a significant reduction of 0.061.
- Hypothetical Benefit: A roughly 6% reduction in the pace of aging, if sustained, could theoretically delay the simultaneous onset of multiple age-related chronic diseases (the Geroscience Hypothesis).
- Systemic Resilience: The 6.33-year reduction in the PhenoAge clock suggests an improvement in the body’s ability to maintain homeostasis under stress.
Critical Analysis and Knowledge Gaps
While the mechanistic data is compelling, several factors limit the immediate translation of these findings into clinical practice:
-
Cohort Age Bias: This study used healthy adults with a mean age of approximately 28 years. It remains unproven whether the same magnitude of effect—or any effect at all—would occur in older adults whose silencing mechanisms for transposable elements are more severely degraded.
-
Absence of Functional Testing: The trial relied entirely on molecular biomarkers (epigenetic clocks) . There was no direct measurement of physical strength, cognitive speed, or organ function to verify that “younger” clocks result in improved physical performance.
-
Exploratory Status: As a post-hoc analysis of studies not originally designed for aging, the results were not corrected for multiple testing . Consequently, these benefits should be viewed as informed speculation that requires validation in prospective, placebo-controlled trials .
3 Likes
Was Magic Johnson taking Descovy? Pictures are from 1980, 1995 and 2024 (yes, lighting conditions, etc). They show him 44 and 29 years older. I’m no judge, so does this look like normal aging to anyone who might be?
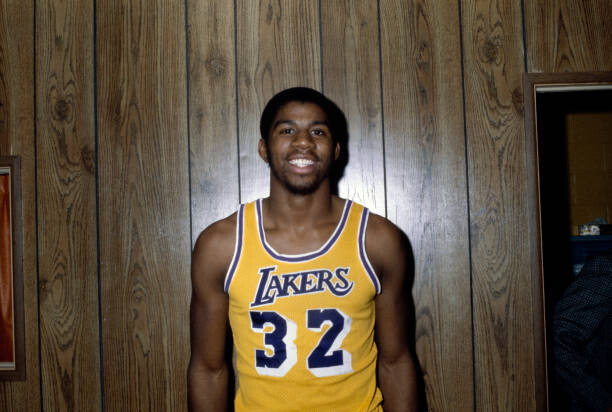
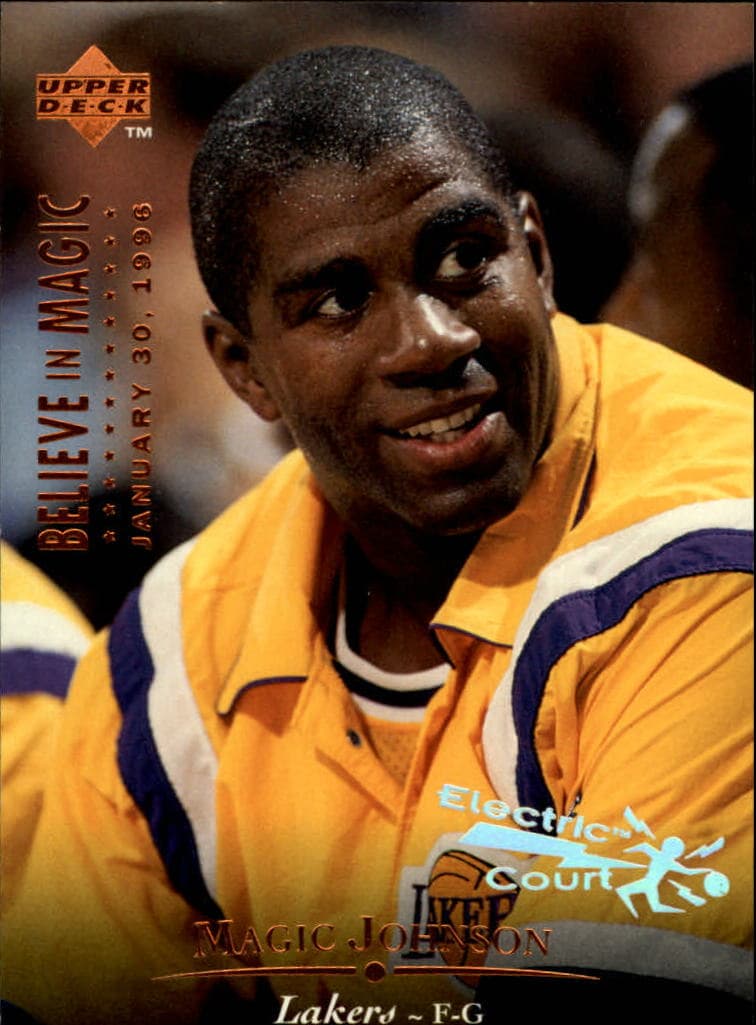

2 Likes
High levels of melanin is the ultimate natural sunscreen!
4 Likes
There’s that. Plus, he never frowns. I trust one of the face experts here will see more.
1 Like
I do have PrEP at home because I am irrationally afraid of HIV but it’s hidden in my household meds cabinet and next to the condoms. The package is unassuming.
3 Likes
Here’s a paper from Japan from 2022 that showed
Resveratrol blocks retrotransposition of LINE-1 through PPAR α and sirtuin-6
https://www.nature.com/articles/s41598-022-11761-0
It was an in vitro trial, however.
3 Likes