Cross-sectional analyses at baseline revealed that higher levels of sex hormone–binding globulin were associated with lower BMI, a lower likelihood of having a history of hypertension, and more favorable lipid-profile and CRP levels
This has made me reconsider my anti-sarcopenia as MK-2866 drastically suppresses SHBG as it’s processed by the liver. Going to do a Tamoxifen PCT exit.
Here’s the proposed mechanism for SHBG and type 2 diabetes:
Our prospective findings for plasma levels of sex hormone–binding globulin levels and risk of type 2 diabetes are consistent with results from previous cross-sectional studies of diabetes.6,8 Sex hormone–binding globulin may play an important role in the pathogenesis of type 2 diabetes, by modulating the biologic effects of sex hormones (testosterone and estrogen) on peripheral tissues (i.e., liver, muscle, and fat). Studies suggest that sex hormones bound to sex hormone–binding globulin may also be biologically active, amplifying their signaling, endocytosis, or overall biologic actions.1–3 For example, sex hormone–binding globulin has been shown to have direct cellular antagonistic properties against estrogen4,32; interaction of sex hormone–binding globulin with the cellular estrogen receptor can trigger a biologic antiestrogen response,4 a form of mediation beyond simple hormone sequestration. Our results may provide a potential explanation of the intriguing divergent effects on the risk of diabetes, observed in two randomized trials, of transdermal estradiol (which elevates plasma glucose levels) and oral estrogen (which lowers glucose levels).33–35 In direct comparisons, transdermal estradiol does not affect sex hormone–binding globulin levels, whereas oral-estrogen therapy favorably increases levels of sex hormone–binding globulin.36–38
Keep in mind there are a lot of disease states that may increase or lower SHBG, the MR study was solely acting on SHBG as far as I can tell (with genetic variant that either increases or decreases SHBG).
So someone could have a high SHBG from a disease which probably nulls the effect. So on an individual level, someone who have a blood test with e.g high SHBG levels, this could be confounded by a disease, which drastically changes the total calculation.
For what’s its worth SHGB jumped up right after beginning E3. It was perhaps the most notable single blood test change. I’ve never done a wash-out test, so its possible my SHBG was just temporarily low at the time of initial dosing, idk. Now I don’t really “think about” E3 anymore, its just part of my regular stack like rapa.
I’m curious to know how you are using E3 if you don’t mind sharing. I’ve recently started 17 alpha E topical with transcutol. I’ve also been considering a topical E3 skin cream.
I alternate weekends (Fri, Sat, Sun) with rapa/E3 at 3mg each day, so about 18mg of E3 and 18mg of Rapa per month. I’m not sure on the systemic bio-availability of creams and hair tonics. I think the E3 creams directly on the genitals (scrotum) might have high absorption, but given the vast unknowns, that route is something I might only try if other options run out when I’ve very old.
The addition of transcutol will enhance the transdermal absorption of 17 alpha E, but as you have said, it’s pretty much a guess. I’m applying it to my scalp since I have some male pattern baldness. It is thought to help with male pattern baldenss through it’s 5 alpha reductase effects. 17 alpha E was wildly successful on male mice in the ITP (+19%), so that’s why I’ve gone with it.
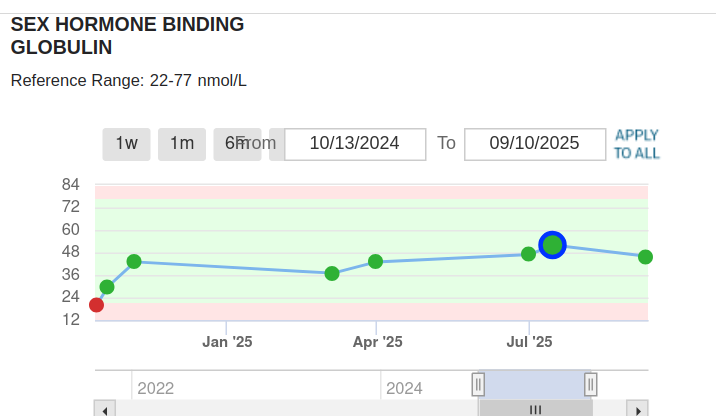
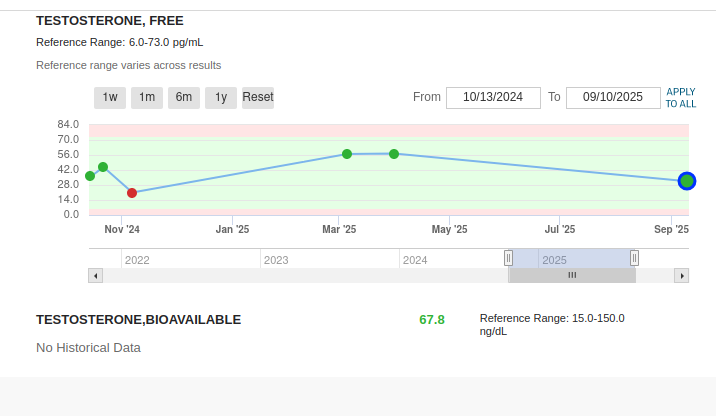
This discussion is helpful for me to realize that a high SHBG is not necessarily a bad thing (actually good). My total T of 358, with SHBG of 82 and low free T is in the context of a 68 year old male with excellent metabolic health (A1C 5.0, fasting insulin 1, BMI 21, VO2 max 46). I have started a boron supplement of 3 mg/day. I will continue to monitor the sex hormones.
Keep in mind it’s actually high SHBG throughout life which is protective, not due to aging.
A natural increase in SHBG with aging is not the protective to the same extent.
So an increase in SHBG without any other reason, including age, is protective. I’m not sure how to discern this.
I’m thinking it’s important it has/is increased by other preventative measures, at least you have that to boost the effect and decrease the chance it’s because of something else.
So it’s a bit tricky. Lustgarten has a good idea of having a total net benefit of markers.
E.g if someone is healthy and has a normal SHBG but does traditionally healthy things or improve their markers, it is under this circumstance if these things increased SHBG that it is particularly good. Making sure anything bad that might increase it is not occurring either, so checking biomarkers that increase SHBG are actually in the optimal range.
Light–moderate alcohol intake is associated with higher SHBG, likely via liver signalling.
• ~1 standard drink/day (or less)
• Do not start drinking for this reason alone
Evidence level: Observational only (not a recommendation)