Actionable Intelligence
-
The Translational Protocol (Rigorous Extrapolation):
-
Human Equivalent Dose (HED): The clinically tested human daily dose is:
-
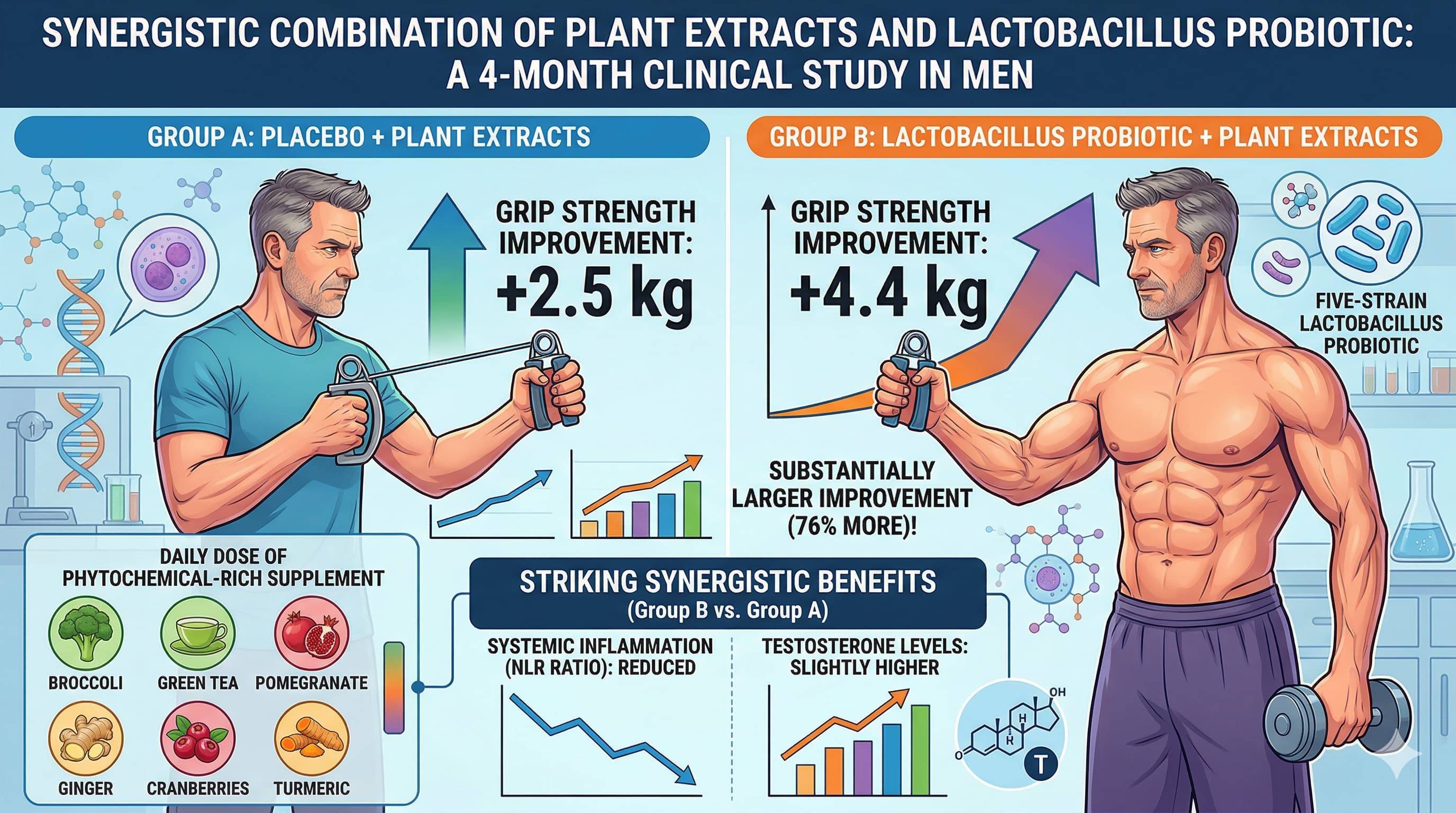
Phytochemicals (2 capsules/day): 300 mg Curcuma longa (standardized to 500 mg curcuminoids), 300 mg Pomegranate (standardized to 500 mg ellagic acid), 300 mg Green tea (standardized to 150 mg EGCG), 300 mg Broccoli, 200 mg Cranberry, and 10 mg Ginger.
-
Probiotics (2 capsules/day): 10 Billion CFU Lactobacillus blend (L. rhamnosus, L. plantarum, L. paracasei, L. bulgaricus, L. lactis), 200 mg Inulin, and 1,000 IU Vitamin D.
-
Pharmacokinetics (PK/PD): Standard curcumin and EGCG have notoriously poor oral bioavailability and rapid systemic clearance. Unformulated curcumin has a plasma half-life of <2 hours, while EGCG peaks in 1-2 hours with only ~1-2% absolute bioavailability. Without lipid matrices (like liposomes) or piperine to inhibit glucuronidation, the primary pharmacological action of these compounds is almost certainly isolated to the local gastrointestinal lumen, acting upon the microbiome before excretion.
-
Safety & Toxicity: * NOAEL / LD50: The NOAEL for curcumin in reproductive toxicity studies is established at 250–320 mg/kg BW/day. EGCG is generally recognized as safe, though the European Food Safety Authority notes rare hepatotoxic signals at doses exceeding 800 mg/day (this trial uses a safe 150 mg dose).
-
CYP450 Interactions: Both curcumin and EGCG are known inducers/inhibitors of hepatic enzymes, specifically inhibiting CYP3A4 and CYP2C9.
-
Biomarker Verification: Neutrophil-to-lymphocyte ratio (NLR) is a crude proxy. To genuinely verify biological target engagement of this protocol, an analyst should measure: 1) hs-CRP and IL-6 for systemic inflammaging, 2) Plasma Urolithin A (to verify if the microbiome is actively converting the pomegranate’s ellagic acid), and 3) Fecal Short-Chain Fatty Acids (SCFAs) to confirm butyrate upregulation.
-
Feasibility & ROI:
-
Sourcing: Highly accessible. The exact supplements used in the trial are commercially available over-the-counter (YourPhyto and YourGutPlus).
-
Cost vs. Effect: The combined protocol costs approximately $45–$55 USD per month. Given the heavy methodological confounders in the trial, the ROI is likely low for individuals already maintaining a diverse, polyphenol-rich diet, but may offer a moderate stop-gap benefit for those with documented gut dysbiosis.
Part 5: The Strategic FAQ
1. Doesn’t the baseline age and strength disparity between the two groups completely invalidate the finding that the probiotic increased grip strength? Yes, it severely confounds the data. The probiotic arm was, on average, 3 years younger and started with a baseline grip strength 5.3 kg heavier than the placebo arm. It is highly probable that the larger total improvement (+4.4 kg vs +2.5 kg) is a reflection of starting with a younger, physically superior cohort rather than a pure outcome of the probiotic intervention.
2. Since testosterone was only measured at the 4-month mark, can the authors genuinely claim the probiotic boosted testosterone? No. This is a glaring methodological hole. Because they did not draw baseline testosterone labs before the trial began, it is mathematically impossible to know if testosterone increased. The 12% higher testosterone level in the probiotic group at month 4 is likely because that cohort was younger from day one.
3. Does the unformulated curcumin in this supplement actually reach systemic circulation to inhibit inflammation in the muscles or joints? Almost certainly not. Without bioavailability enhancers (like piperine or phytosome technologies), raw Curcuma longa extract is rapidly conjugated in the liver and excreted. However, this is precisely why it pairs well with probiotics: the unabsorbed polyphenols remain in the gut lumen, acting as metabolic fuel (prebiotics) for the Lactobacillus strains.
4. How does this protocol interact with Rapamycin and PDE5 inhibitors? **[Interaction Check - Red Flag]:**Curcumin and EGCG are established inhibitors of the CYP3A4 enzyme in the liver. Both Rapamycin and PDE5 inhibitors (e.g., tadalafil) are heavily metabolized by CYP3A4. Taking this phytochemical supplement concurrently with Rapamycin could suppress drug clearance, unexpectedly spiking Rapamycin trough levels and increasing the risk of immunosuppression or mTORC2 inhibition.
5. How does this protocol interact with Metformin, Acarbose, and SGLT2 inhibitors? [Interaction Check]: Both Curcumin and EGCG activate AMPK, which is the primary mechanism of Metformin; stacking them may yield diminishing returns or increase the risk of gastrointestinal distress. Acarbose directly alters the microbiome by delaying carbohydrate absorption—this could aggressively amplify the fermentation of the prebiotic inulin and phytochemicals in the colon, potentially causing severe bloating. SGLT2 inhibitors have no known direct CYP interactions with these plant compounds, but shared risks of mild dehydration should be monitored.
6. How does this protocol interact with 17-alpha estradiol (17aE2)? [Interaction Check]: 17aE2 is metabolized through various hepatic pathways, but the specific impact of EGCG/curcumin-induced CYP3A4 inhibition on 17aE2’s clearance requires cautious observation. Given the poor systemic absorption of the phytochemicals in this specific unformulated dose, the interaction risk is likely low, but concurrent administration should be spaced out.
7. Does taking pomegranate extract guarantee the anti-aging benefits of Urolithin A? No. Pomegranate provides ellagic acid, but humans lack the enzymes to convert it to the mitochondrial-enhancing compound Urolithin A. This conversion relies entirely on possessing specific gut bacteria (often Gordonibacter species). If a patient’s microbiome lacks these specific “Urolithin A producers,” the pomegranate extract will yield minimal mitochondrial benefit regardless of the Lactobacillus provided in this trial.
8. Why did the researchers use this specific 5-strain Lactobacillus blend instead of targeted SCFA-producing strains? The researchers explicitly chose a commercially available supplement with prior Phase I safety data rather than engineering a bespoke longevity probiotic. Lactobacillus strains are excellent at breaking down plant phenols, but they are not the primary producers of butyrate (the most beneficial SCFA for gut lining health and longevity).
9. Is a 4-month timeframe long enough to measure actual muscle hypertrophy from a gut intervention? No. True accrual of contractile muscle tissue in a 74-year-old population takes extensive time and intense mechanical loading. The rapid improvement in grip strength observed is much more likely due to neuromuscular adaptation, a reduction in joint inflammation (arthralgia) allowing the men to squeeze harder without pain, or an improvement in overall systemic energy.
10. If a patient stops taking the probiotic, will the strength and inflammatory benefits persist? No. Exogenous Lactobacillus probiotics rarely colonize the adult gut permanently. They are “tourist” bacteria that exert transient effects while passing through the gastrointestinal tract. If supplementation ceases, the microbiome will revert to its baseline state within 1 to 3 weeks, and the secondary anti-inflammatory benefits will dissipate.