There’s a lot of talk of how to use grapefruit juice to magnify rapamycin in the body. But I’m sensitive to the rapa and still working up to 6mg/ weekly.
I love red ruby grapefruit and just got my first bag of the season, which I’ve been eagerly awaiting.
How much of a buffer do you give between the rapa and grapefruit?
I also eat oranges and understand some of those can have an effect?
It’s going to be an issue. And, it’s not just with rapamycin, it’s with many medications. You likely want to avoid grapefruits for a number of days before rapamycin dosing… see this thread, Improve Bioavailability of Rapamycin (2)
and this explaination from Gemini.ai
Executive Summary: The “Grapefruit Effect” Timeline
For a user optimizing rapamycin (sirolimus) for longevity, the interaction with grapefruit is profound and prolonged due to the specific mechanism of “suicide inhibition.”
Time to Peak Inhibition:2–4 hours after ingestion.
Time to Minimal Inhibition (Return to Baseline):72 hours (3 days) for significant recovery; up to 7 days for complete return to baseline.
Impact on Rapamycin: Increases bioavailability by 350% to 500% (3.5x to 5x multiplier), effectively turning a low dose into a high therapeutic (or toxic) dose.
1. Mechanism of Action: “Suicide Inhibition”
To understand the duration, one must understand the unique mechanism. Grapefruit does not merely “occupy” the CYP3A4 enzyme temporarily; it destroys it.
Active Compounds: Furanocoumarins (specifically 6’,7’-dihydroxybergamottin and bergamottin).
The Process: These compounds act as mechanism-based inhibitors (suicide substrates). When intestinal CYP3A4 attempts to metabolize them, the compounds are converted into a reactive intermediate that covalently bonds to the enzyme, permanently inactivating it.
The Consequence: The body cannot “un-block” the enzyme. To restore metabolic function, the enterocytes (intestinal cells) must transcribe and synthesize entirely new CYP3A4 proteins. This biological “re-manufacturing” process dictates the prolonged recovery time.
Note: This inhibition occurs primarily in the intestine, not the liver. This essentially removes the “first-pass metabolism” barrier, allowing a flood of unmetabolized rapamycin to enter the bloodstream.
2. Detailed Timeline of Inhibition
The following table outlines the lifecycle of CYP3A4 inhibition following a single serving (approx. 200–300 mL) of grapefruit juice.
Maximal suppression of enzyme activity. Drug absorption potential is highest here.
Partial Recovery
24 hours
~50% of enzyme activity is restored as new enzymes are synthesized. Interaction risk remains high.
Significant Recovery
48 – 72 hours
Enzyme activity returns to near-normal levels for most individuals.
Complete Baseline
3 – 7 days
Full restoration of CYP3A4 activity, ensuring no residual interaction.
3. Impact on Rapamycin (Sirolimus) Pharmacokinetics
Rapamycin has poor oral bioavailability (~14%) because intestinal CYP3A4 and P-glycoprotein (efflux pump) aggressively filter it out before it reaches systemic circulation. Grapefruit juice neutralizes this filter.
Quantitative Impact
AUC (Area Under the Curve): Total drug exposure increases by 350% (3.5-fold) on average, with some studies showing increases up to 500%.
Cmax (Peak Concentration): Peak blood levels can increase by 300% to 500%.
Actionable Translation: Taking 1 mg of rapamycin with grapefruit juice is pharmacokinetically equivalent to taking approximately 3.5 mg to 5 mg with water.
Implications for Longevity Protocols
In longevity medicine, rapamycin is often dosed once weekly (pulsed) to inhibit mTORC1 while minimizing mTORC2 inhibition and side effects (e.g., immunosuppression, glucose dysregulation).
Loss of Precision: Because the level of furanocoumarins varies wildly between individual grapefruits (and juice batches), using grapefruit to “boost” your dose is unpredictable. You cannot reliably titrate the multiplier effect.
Half-Life Extension: Rapamycin has a half-life of ~60 hours. Inhibiting CYP3A4 not only increases the peak but may extend the elimination phase, potentially causing the drug to accumulate and “bleed” into the next dosing window, violating the “clean” on/off cycle required for longevity benefits.
The “Safety Window”: If you consume grapefruit, you should ideally wait 72 hours before taking your rapamycin dose to ensure the “multiplier effect” has dissipated.
Summary of Actionable Insights
Avoidance Window: To guarantee standard dosing accuracy, avoid grapefruit for 3 days prior to your weekly rapamycin dose.
Intentional Boosting: While some oncologists use grapefruit juice to lower the cost of sirolimus for cancer patients (who take high daily doses), this is generally ill-advised for longevity users due to the high variability in furanocoumarin content. If cost is a barrier, generic ketoconazole is sometimes used as a more consistent booster, though this adds pharmaceutical complexity.
Dietary Vigilance: Be aware that other citrus fruits like Seville oranges (often used in marmalade) and pomelos contain similar furanocoumarins and will induce the same CYP3A4 destruction.
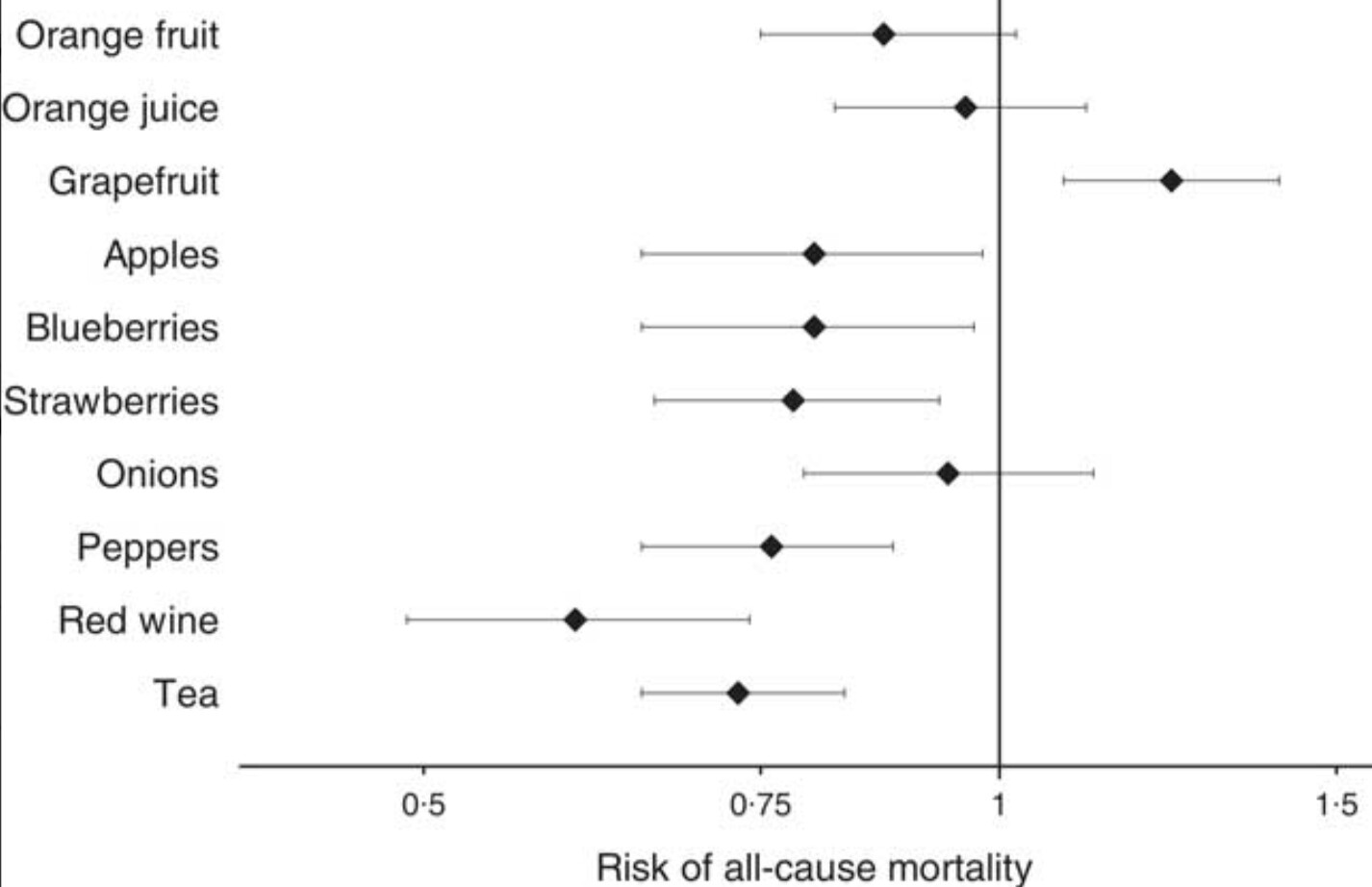
I assume you thoroughly researched health effects of consuming grapefruit? I like the taste, but gave it up based on the possible effect on all cause mortality and complicated interactions with drugs, supplements and food. There are beneficial polyphenols, but what’s the ultimate balance? In the end, the juice is just not worth the squeeze for me, shameless pun. But, of course to each their own. YMMV.
As I have posted I have been using ruby red grapefruit juice with my weekly dose of rapamycin to produce a high dose. I have been doing this for 4 years now, and it hasn’t killed me yet. And the massive accidental/suicidal dose didn’t kill anyone either.
I am still in Dr. Blosklonny’s camp that the highest tolerable dosage is best.
Dr. Blagosklonny ultimately recommended a personalized, maximal tolerated dose (MTD) administered intermittently as the optimal approach for longevity. His reasoning was based on evidence in mice, which showed a dose-dependent increase in lifespan with higher doses. "In mice, the higher the dose, the longer the lifespan. Therefore, in humans, the highest dose that does not yet cause unacceptable side effects (maximal tolerated dose) may be optimal for longevity. If (unacceptable) side effects develop, the dose should be decreased. In other words, anti-aging doses are maximal doses without side effects in a particular person. "
As a result, I am still ticking at 85, pain-free and disease-free. I have never had a cold, flu, or any other illness in the last four years. The extended wound healing time is exaggerated. Maybe a little longer for cuts, but that is hard to measure individually.
So, despite AI’s advice, I will continue to follow Dr. Blosklonny’s advice and take the highest tolerable dose. However, I don’t know if this is good advice for younger people. Who knows, perhaps taking larger doses in younger years might be the best life extension protocol. No one knows.
Thank you so much. So no grapefruit for 72 hours BEFORE my weekly dose. My window is clear for this week’s dose. But what about after the dose? Can one wait a couple of hours (I’m thinking more like 24 hours to be cautious) and eat grapefruit again as long as you pause 72 hours before the next dose?
I’m not sure how much to weigh this. There are known interactions with many prescriptions, but outside of those, I suspect it’s one like eggs which looked like bad foods for a while and are now considered good.
Clearly, however, if I’m staying on rapa, my consumption will be limited.
Well, from what I can gather, that potential 7 day window for some users is a real risk, so I guess I’ll give my grapefruit away. I’m tempted to eat one on the day that is three days removed in both directions. But we’ll see. Thank you.
This is not true, at least not as a generalization. In some ways you actually get a more predictable absorption if you ingest high doses of grapefruit juice shortly before taking rapamycin. At low doses of grapefruit juice the variation will be unpredictable and will vary widely. At high doses the opposite is true. This is because you can only inhibit the CYP3A4 so much. If you need x amount of CYP3A4 inhibitory compounds in grapefruit to inhibit your CYP3A4 by close to 100% then if 50 ml of grapefruit gives you an average of 0.5x of the compounds but it ranges from 0.2-0.7x then the inhibition is going to vary widely if you drink 50 ml of grapefruit juice. If you drink 100 ml you would get 1x (range 0.4-1.4x) and if you drink 200 ml you would get 2x (range 0.8-2.8x). Even at the lower end of the range you’ll get close to 100% inhibition even with a batch of grapefruit that contains relativel little of the CYP3A4 inhibitory compounds. But you’ll never get more than 100% inhibition. Because of this, if you take a fairly high dose of grapefruit (a good bit more than what is likely to inhibit the CYP3A4 enzymes by a decent amount on average) then you can almost guarantee that you’ll get a fairly strong CYP3A4 inhibition.
Note: the x numbers I used above are not accurate, I just used them to illustrate a point.
I agree. Just take a large amount of grapefruit juice to inhibit the CYP3A4. Actually, this is pretty reliable from what I have read. But I really don’t care if its effect as a multiplier of my rapamycin dose is 2X or 4X because I am in the max tolerable dose camp. Currently I am taking 8 mg of rapamycin with at least 12 oz of ruby red grapefruit juice ~ 2+ hours after drinking the juice. I tolerate this well and enjoy the effect. I understand that not everybody can tolerate this large of a dose. But according to ChatGPT 5, to achieve “saturation” (near-max) effect 12 oz should do it with most grapefruit juices.
Rule of thumb: ~200–250 mL (8.45 fl oz.) gets you near the “ceiling” for many people/drugs; more in that sitting usually doesn’t add much. PMC+1
Mechanistically, grapefruit juice reduces intestinal (enterocyte) CYP3A4 substantially; reductions have been observed after repeated intake and even “markedly reduced” levels can be seen within hours after a single glass in some reports. PMC