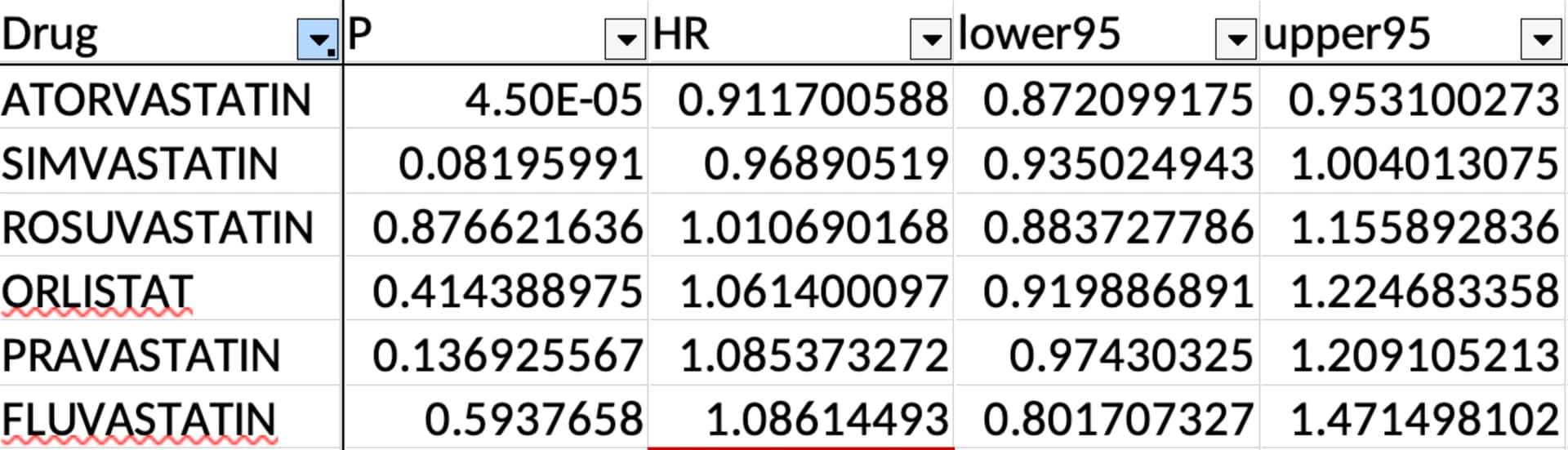
Also, among statins, only atorvastatin had a significant positive effect on mortality:
Importantly, we identified 14 drugs that increased lifespan, compared to health matched controls (Figure 2, Data Table 2), independently of current smoking, cancer diagnosis, diabetes, gender, and age at recruitment. These included notably the statin Atorvastatin (HR 0.91, CI 0.87-0.95), the PDE5 inhibitor Sildenafil (HR 0.85, CI 0.78-0.93), the anti-inflammatory drug Naproxen (HR 0.90, CI 0.85- 0.96), and the estrogen related drugs Estraderm (HR 0.67, CI 0.51-0.88), Vagifem (HR 0.73, CI 0.59-0.91), Estriol (HR 0.74, CI 0.60-0.92) and Estradiol (HR 0.75, CI 0.59-0.95). Others included, Lymecycline, Otomize, Marvelon, and 2 vaccines (Avaxim, Revaxis).
Statins as a class had a tiny positive effect: “Statins (HR 0.97, CI 0.94-1.00)”
Does it mean that some statins have a detrimental effect? We really need the whole dataset to conclude… But in the meantime, should people prefer atorvastatin to other statins?
I also find it interesting that after simvastatin failed the ITP, they decided to test for atorvastatin.
(and what are the 2 drugs not listed out of the 14?!)