i bought 20 pills from NIBA healthcare of India. One pill costs $7.
try 5mg Everolimus yesterday with grapefruit juice, no side effect, feels good like the first time i took sirolimus months ago. I will try more times.
“One of the key differences between sirolimus and everolimus in these studies was that at therapeutically relevant concentrations everolimus, but not sirolimus, could distribute into brain mitochondria”. On the other hand, it said “everolimus is markedly more potent than sirolimus in inhibiting mTORC2 formation”.
Looks like it has both positive and negative effects. May be you just need only few mg of everolimus to reach the brain, you dont need 20 mg of sirolimus to cross BBB.
“There is also evidence that everolimus alone, but not sirolimus, stimulates mitochondrial oxidation. In rat brain slices, in contrast to sirolimus which reduced high-energy metabolism, everolimus stimulated high-energy metabolism as indicated by significantly higher phosphocreatine and NAD/NADH concentrations.”
I’m not sure stimulating high-energy metabolism is a good thing for anti-aging effects.
Yes, not clear which is positive, and which is negative.
My view is that biochemical pathways are generally too complicated to base predictions on (this is esp. true for massively complicated pathways like NAD-related pathways).
So theory-less empirical evidence is always what I prefer. We have that (albeit mostly in mice) with rapamycin, so I’m inclined to stick with rapamycin.
Clinical remission of an inoperable malignant insulinoma by the combination treatment with octreotide and everolimus (2018)
This is an n=1 patient with existing cancer, treated with Everolimus 10mg/day, albeit dual drug intervention.
Abstract
"We report a 52-year-old woman with inoperable malignant insulinoma with multiple liver metastases. Histological examination of biopsy specimens from the pancreatic and hepatic lesions revealed pancreatic neuroendocrine tumor (pNET), G2. The tumor cells were positive for somatostatin receptor (SSTR) 2, 5, and the mammalian target of rapamycin (mTOR). Monthly intramuscular administration of octreotide LAR and once-daily oral administration of everolimus combination treatment markedly reduced the sizes of liver metastases, and hypoglycemia was
well controlled. Combination treatment with somatostatin analog and mTOR inhibitor may be another effective approach in inoperable metastatic malignant insulinoma.
After 20 months of combination treatment with octreotide and everolimus, all of the metastatic lesions of the liver were reduced in size, and many of those had disappeared. In addition, swollen lymph nodes around the pancreatic tumor had also disappeared."
20+ months at 10mg/day Everolimus, that is a high and long dosing exposure, likely high plasma and AUC levels. No data was reported of any side effects concerns.
From the paper: Clinical remission of an inoperable malignant insulinoma by the combination treatment with octreotide and everolimus (2018)
Recently, everolimus, an orally active mammalian target of rapamycin (mTOR) inhibitor, has been shown to have antitumor growth effects in patients with pNET.3 The protein of mTOR is a serine/threonine kinase that regulates cell growth, proliferation, and metabolism. In pNETs, the expression of mTOR protein is upregulated.9 The expression and activity of mTOR and its downstream targets such as 4EBP1, S6, and eIF4E are strongly dependent on enhanced proliferative capacity and metastatic sta- tus in gastroenteropancreatic neuroendocrine foregut and mid- gut tumors. Evidence from preclinical studies suggests that the combination of pasireotide and everolimus may be synergistic by dual inhibition of insulin-like growth factor-1 (IGF-1) and mTOR signaling.10 The combination treatment may be more effective than each treatment. The maintenance therapy with somatostatin analog and mTOR inhibitor combination treatment may play a significant role in tumor control in patients with advanced NET, unless hyperglycemia induced. Further studies in larger numbers of insulinoma patients are required to support this suggestion.
4 | CONCLUSION
We reported a case of inoperable metastatic malignant insulinoma, in which liver metastases were markedly reduced and hypoglyce- mia was well controlled by monthly intramuscular administration of octreotide LAR and once-daily oral administration of everolimus. Combination treatment with somatostatin analog and mTOR inhibi- tor may be another effective approach in inoperable metastatic malignant insulinoma.
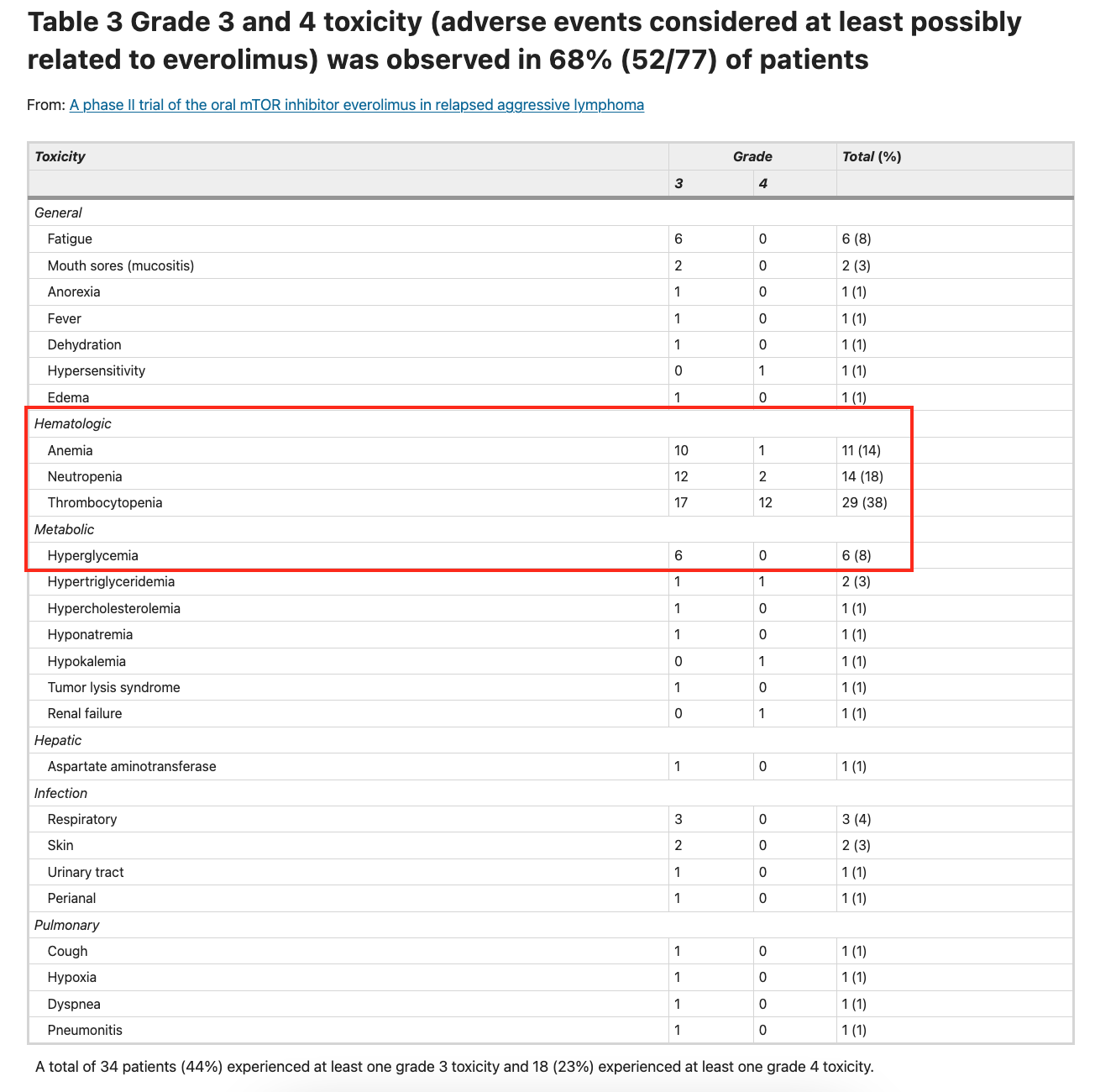
In another large study, 10 mg/day Everolimus, some very strong side effects. I would surmise most healthy people would find many of these side effects intolerable. There’s a comment about adding a statin for hyperlipedemia, although a very minor grade 3/4 side effect incidence rate.
"42 patients (55%) experienced a grade 3 or higher hematologic toxicity (35% grade 3 and 19% grade 4). Grade 3 or 4 anemia, neutropenia and thrombocytopenia occurred in 14, 18 and 38% of the patients, respectively. A total of 22 patients (29%) experienced a grade 3 or higher non-hematologic toxicity (23% grade 3 and 5% grade 4). Overall, 52 patients (68%) had at least one grade 3/4 toxicity at least possibly related to everolimus. Although most patients experienced toxicity, as described in table 3, the incidence of most of these complications was low and they were manageable with dose interruptions and dose reductions. Thrombocytopenia was the cause of most dose reductions and was rapidly reversible with drug delays of typically 1 week. Three patients experienced grade 3 respiratory tract infection. Two additional patients had grade 3 pulmonary toxicity—one with cough and the other with dyspnea, hypoxia and non-infectious pneumonitis. Most all of these toxicities can be managed with dose interruption and dose reduction after the toxicity resolves. In the case of hyperlipidemia, the addition of a statin drug is often required to maintain mTOR inhibitor dose intensity, especially if the patient has an antitumor response and will be on the drug for an extended period of time
I don’t think anyone is recommending 10mg per DAY for cancer prevention / anti-aging. And, it seems important to note also, even if someone did want to do this:
At this time I still believe, given all the data I’ve seen, that it is a reasonable strategy for anti-aging would be to pulse dose everolimus (alternating with rapamycin) at somewhere between 5mg and 20mg per week. The primary benefit, I believe, with the everolimus, is the better blood brain barrier penetration and therefore brain autophagy.
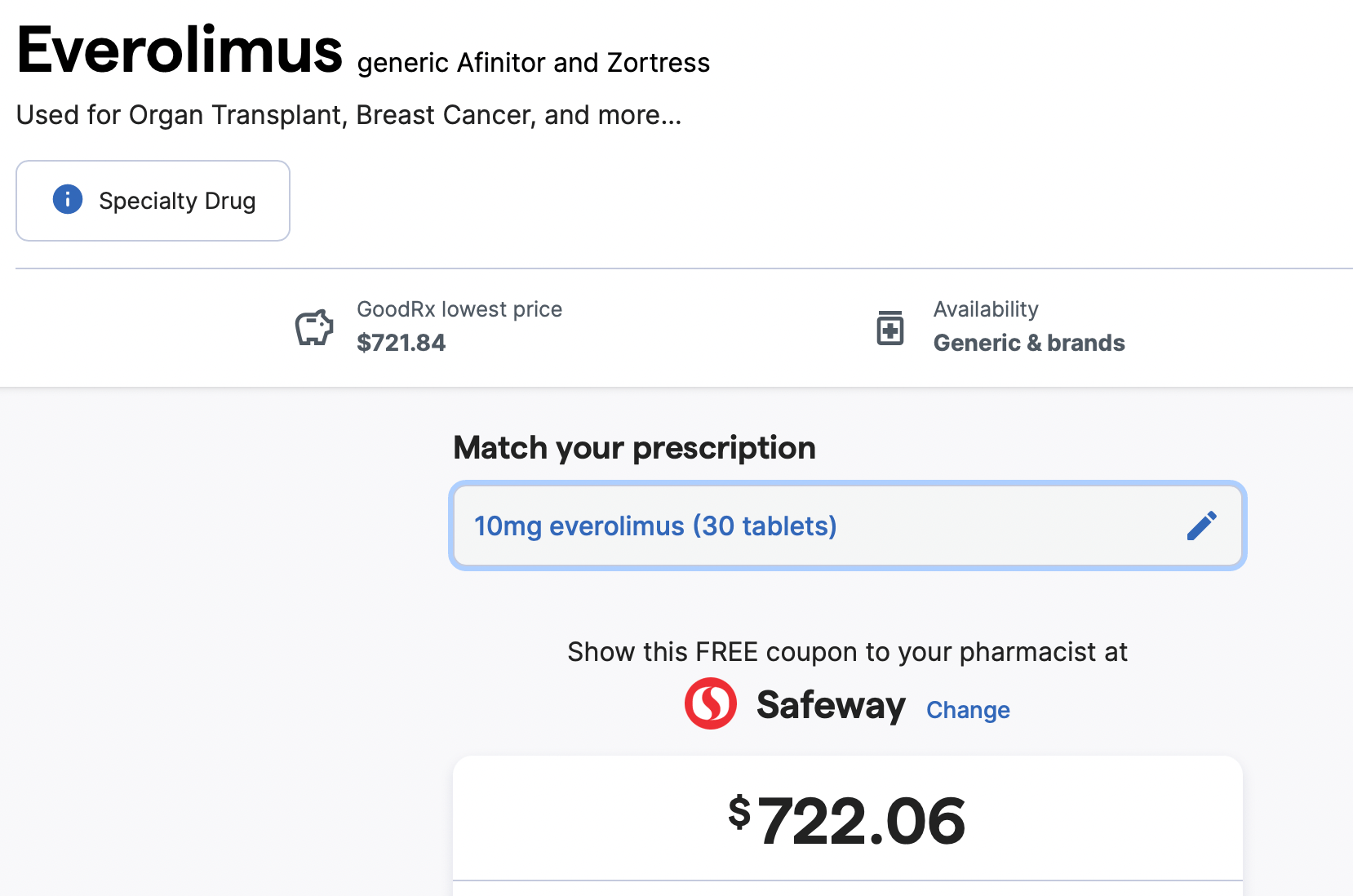
@rapadmin Indeed, lower dose/weekly very much tolerable, but how much mTOR inhibition?? Did you say elsewhere Everolimus off patent, is it populating the Indian generic vendors offering?