Hi all re high LDL vs CHD risk vs studies… Tnx for asks and contradictions. Lots of fuzziness and per person variabilities in this area.
-
(My views) Finally major Med Magazines authors are finally writing that some percent of studies even Mag peer reviewed are non-reproducable or Statistical math trickery was used to find a small benefit.
-
There are alot of past studies on LDL/Statins/CHD risk. How many are “directed out come”?
-
We pay $$ to go to confs every yr and take the latest from the on stage folks who study and find the faults in past studies etc. I can’t in the 1st person discuss one study vs another. I filtered and posted the summary of what I heard from the stage (Denver Low carb 2023, Boca FL low carb 2023)
-
We are all responsible for coming to our own conclusions re best path for our health. I certainly respect anyones views that may contradict what I have summarized.
-
I apologize for not giving URLs to latest or best structured CHD / statin / LDL studies…
-
I can recommend as money and time well spent going to the Feb +/- Boca Raton FL Metabolic Health conf and March ish Denver Metabolic Health conf. I see the same speakers at San Diego in a month I think. Seen similar speakers at KetoCon but I’m less keen on public facing confs. I prefer Researchers/MDs in the audience focused.
-
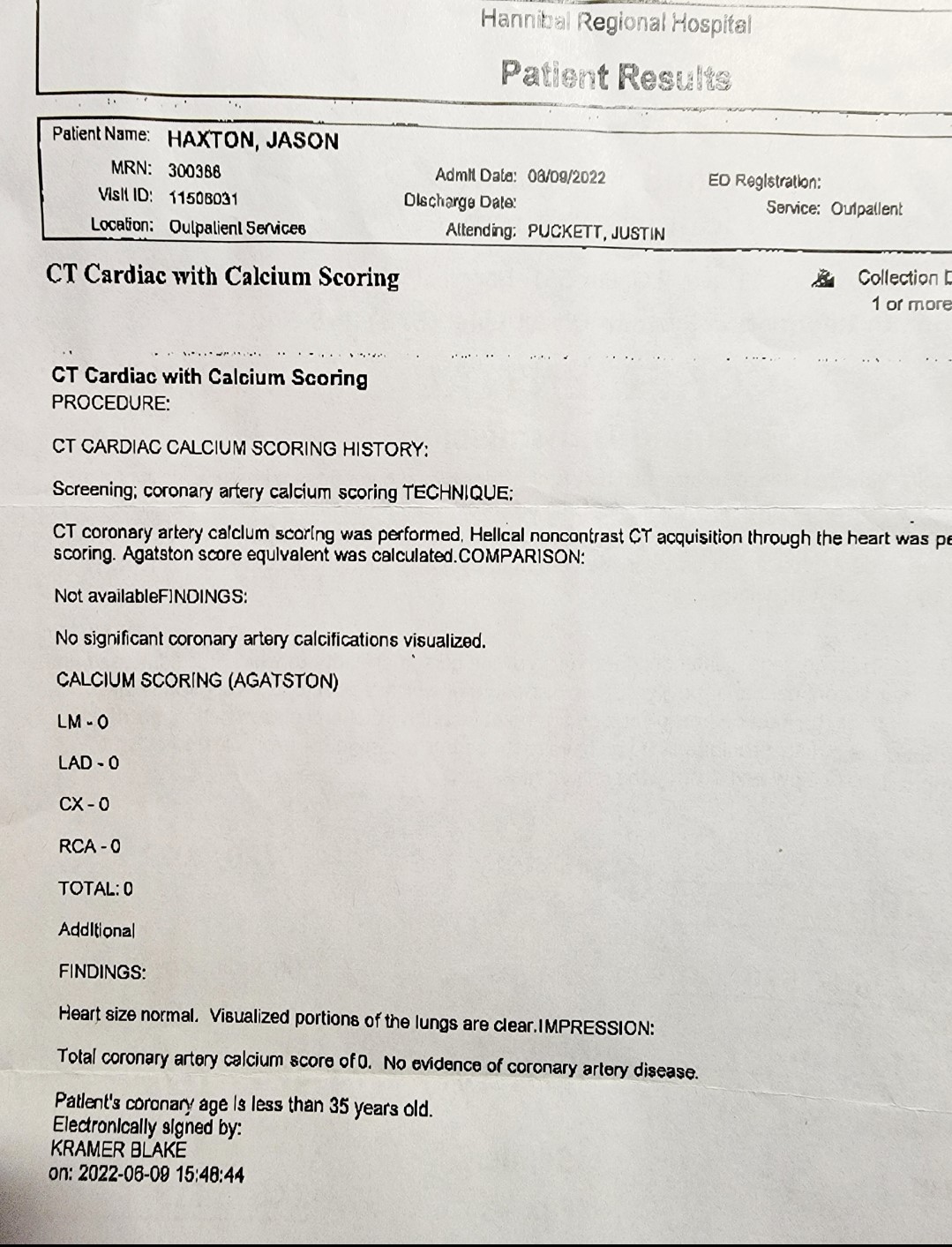
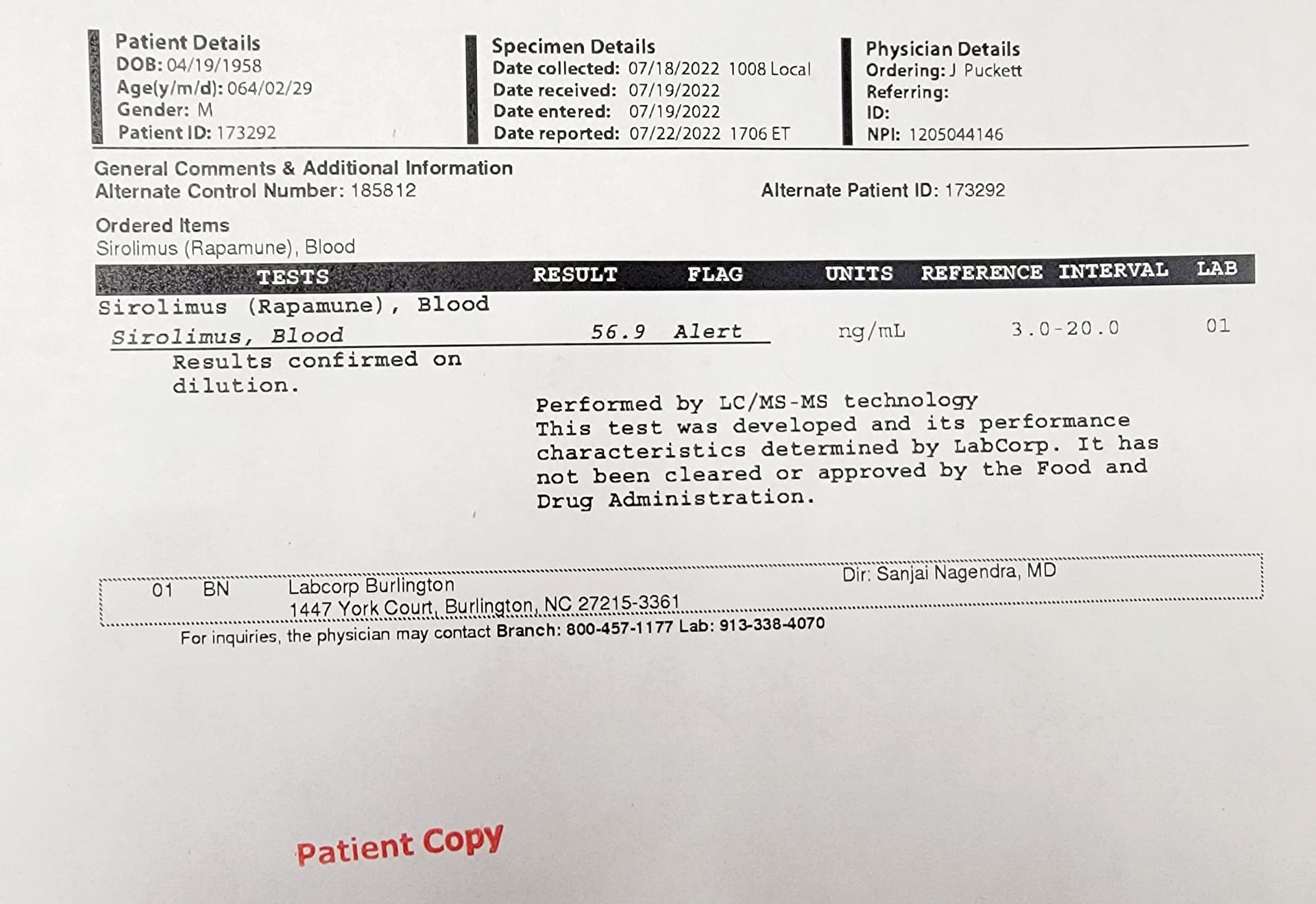
Other threads mention some here are experiencing Poly-Pharma. Well that describes my kitchen sink protocol which I’m certain some percent for me; is counter protuctive and some not good or bad. All I can do is blood test and body scan. So far I havent given myself cancer, artharitis, pre mature death, knocked my hair out etc. I have decent blood tests and very good calcium.
I’m looking at that Millionaire anti aging self experimenter (??) and trying to figure what age tests he’s been taking. Since there’s a bunch of age tests some better then others. I don’t have personal data on my effective age or rate of aging (??). Lance Hitchings (a youtuber) is starting an insiders group so I should be hooking into my missing tests of effective age vs chronological and the latest metric; “rate of aging”. That Millionaire’s rate of aging is 0.71, his $$$ has successfully puts him as lowest ager on his website. Good for him!!!
My practice; test test test including multi-calcium tests and look for changes good vs bad, then possibly make changes.
Wishing all well, Curt