Yes but the stuff that comes up if I google that is dubious articles that do not give any evidence that oxalate toxicity is real. A quick search on PubMed brings up nothing suggesting that oxalate intake causes toxicity.
Also if someone removes vegetables or foods high in oxalate from the diet and experiences improvements in health that doesn’t necessarily mean it was the reduction in oxalates that resulted in the improvement. There could be a number of other reasons for that.
I don’t know about oxalate being toxic for the average person but I get calcium oxalate kidney stones if I don’t manage my intake closely. Apparently some antibiotics can deplete the gut bacteria that help us break down oxalate. My oxalate issues started from a 50 day course of levaquin in the late 90’s after a body fluid exposure at work. It literally took years of going to doctors before anyone took me seriously, analyzed my stones and advised a low oxalate diet. I’m glad it’s becoming more recognized so others hopefully don’t have to suffer needlessly like I did. It does seem like it might be becoming a bit of a fad like gluten free has in people who don’t necessarily need to be so restrictive though.
If one wishes to benefit from the maximum dose of rapamycin with minimum side effects and the minimum risk of rebound, would it not make sense to have a biweekly dosing that starts with high “tolerable” dose week one, and a very low “maintenance dose” week two?
I don’t think I want to wait for evidence of rebound, unless there is a benign marker available to me.
Recently I had been on a very high dose (6 mg rapa + ketoconazole) triweekly (once every three weeks) schedule, thinking it was best to have total wash out between doses. I lowered to 5mg + keto after a UTI, which is still considered a high dose.
However, at this point, (based on lab results) my risk of a cardiac event appears to be low whereas my risk of cancer seems high (10 pack years of smoking, past exposure to high levels of asbestos dust, previous melanomas, grandfather died of prostate cancer).
So by avoiding the extreme swings in serum rapamycin, I believe the likelihood of rebound is lessened as is the development of new malignancies.
Thanks for this. I see the NO/eNOS pathway for producing nitric oxide is up-regulated with Rapa. That is excellent news. What I’ve learned recently is once people get to 60yo, their ability to produce NO via eNOS is diminished by as much as 85%. This obviously impacts CVD in addition to blood pressure, immune function, and much more. I will have a podcast interview on this topic coming out soon.
What I have been told is that viagra (and the like) does not increase NO but makes the NO you have work better. This is an explanation for why viagra does not work (for ED) for men with NO that is very low; they don’t have enough NO to get the effect.
The best way is through diet. Arugula, beets, celery….with nitrates. Also have to use test strips to confirm your oral biome is converting nitrate to nitrite. As we age, the arginine/citrulline + eNOS doesn’t work as well. The diet pathway does work as long as you don’t kill your oral microbiome (antiseptic mouthwash, etc).
Dr Nathan Bryant has lots of good NO research. Heard him talk at 2 conf’s. Im just the messanger:
Stop using antiseptic mouth wash and tooth pastes. No tooth paste with flouride. The oral micro biome is the biggest generator of NO.
Eating some sources of nitrates + natural oral micro biome creates NO.
The arginine pathway (per Bryant) is weak and not worth taking citurline/argine.
Cialis at 2.5mg / day is a healthful protocol. Have seen daily or every other day use of PDE blockers in antii aging protocols. Bryan Johnson is prob too young to need PDE blockers a guess of course.
I need 2.5mg - 5mg of cialis daily for solid erections and don’t use antiseptic anything and take a NO booster product. Many on amazon. Even with the NO booster I still need a PDE blocker.
Even with rapa I still need cialis using erection ease and hardness as the yard stick. (sort of a joke)… Just my N of 1 test whether rapa obviates the need for a PDE blocker. I still need one.
A bunch of videos. One talk to RAAD included women as beneficuaries of a PDE blocker.
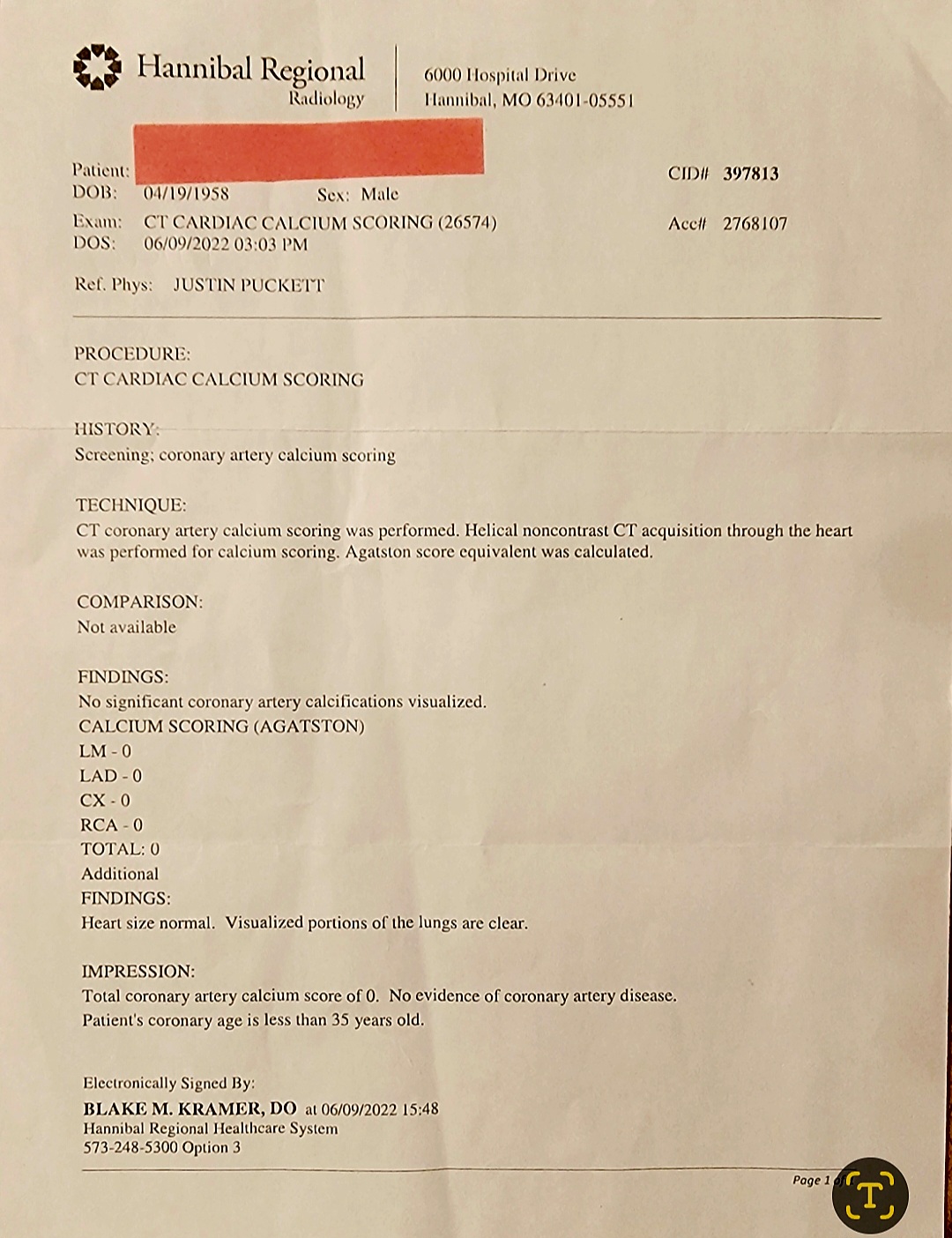
Hello - It is a giant CT scanner… they run you thorugh it… breath… stop breathing - images taken… scoot you in and out… breath… stop breathing … scoot you in and out of the machine.
That’s it – done in a few minutes. NO real prep… maybe don’t exercise of eat 12 hours before test.
My mom’s side passed genetically to me familial hypercholerolaemia. Always had LDL- C above the 130 norm… sometimes 170 last few years. That said, no heart issues back generations (we are Czechoslovakian).All long-lived… healthy. About 13 years ago my family doctor suggested statins… told her I would change my eating habits. Was easier to not see her again. Truth.
Actually in my research with familial hypercholerolaemia… diet, statins and exercise has little improvement effect.
After my workout every other day I have steak, whole milk and a loaded potato. That is going on 6 years straight. And, steak…saturated fat and whole milk has been my regular go to food since college and me being on my own.
Have seen my veins really open up and feel my pulse pumping throughout my body since starting rapamycin 3 years ago.
No secret… dumb luck… familial hypercholerolaemia might serve a person as a phenotype.
Really curious to retake it next again… June 2024.