
Lancet:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)01296-0/abstract
I am surprised it is ranked so high.
My own take is that it is mainly related to:
“Social Isolation: Hearing loss can lead to social isolation and loneliness, as individuals may withdraw from social interactions due to difficulty in communication. Social isolation is a known risk factor for cognitive decline and dementia.”
Almost all older people experience some hearing loss. Perhaps it would be better to be a little more proactive in getting a hearing aid before we constantly ask people to repeat themselves.
Hearing loss is controversial. Some researchers think it is an early symptom rather than a risk factor. Although it could be both: an early symptom that left untreated (no hearing aid) leads to more social isolation, less cognitive stimulation and therefore accelerates decline.
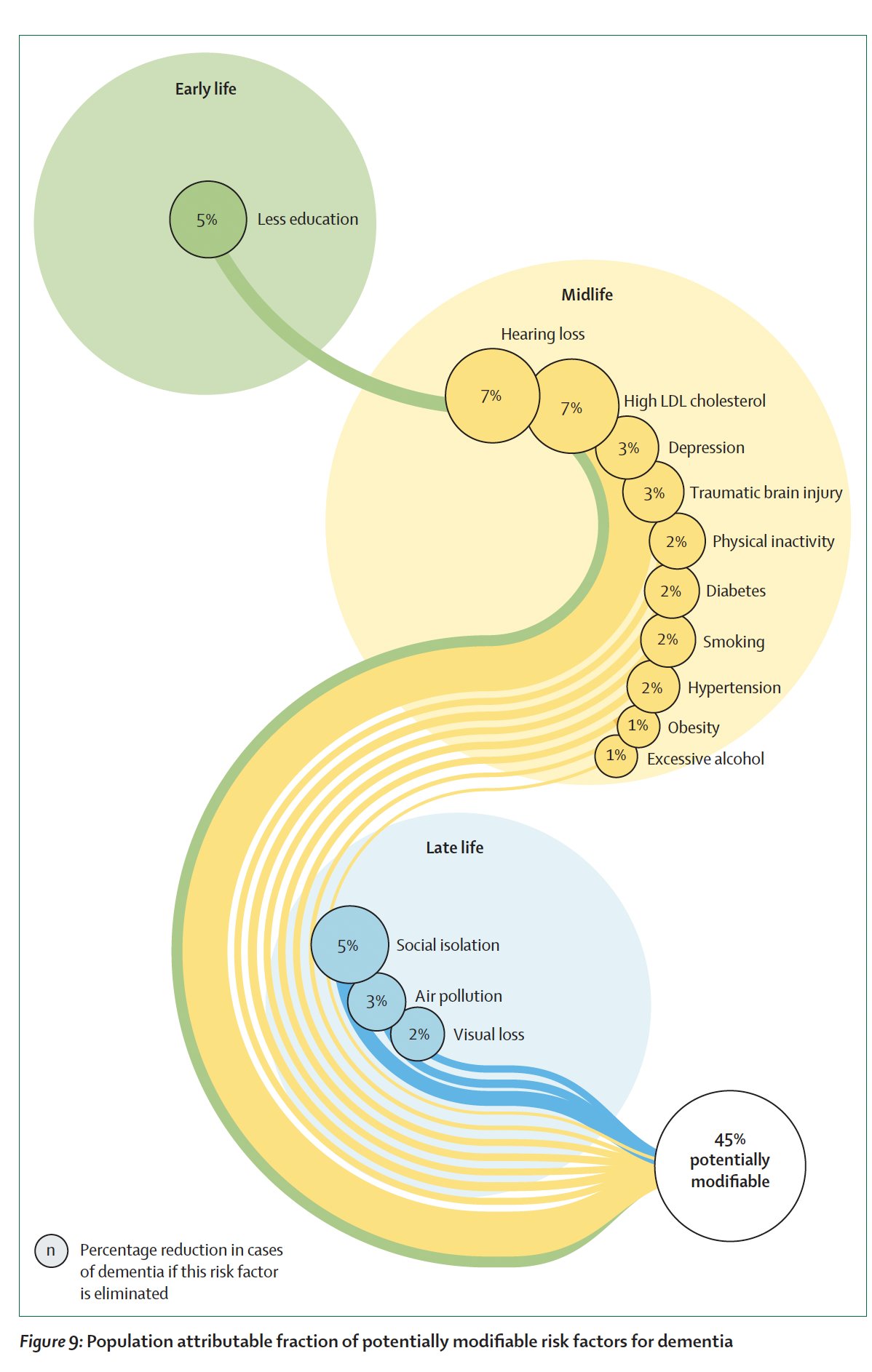
The other risk factors are not surprising. I wonder if they used 140 mmHg or 130 mmHg for “Hypertension”. Using a more restrictive definition might increase the importance of this risk factor. Similarly they cite (ref 195) blood pressure variability, that is probably more important than the average blood pressure, but it’s not on the graph. I would not be surprised if in the future “Blood pressure dysregulation” was ~5%. Same for “Diabetes”, they probably used HbA1c > 6.5%. But people with pre diabetes or just increased HOMA-IR already have an increased risk of dementia. So similarly if they used the broader “Insulin resistance” instead of “Diabetes” it might be ~5%.
Things that are absent and might be modifiable risk factors: erectile dysfunction, vitamin deficiency (esp. B12?), ultra processed food consumption, insomnia (but do we have good treatments?), lack of vaccinations.
With all the above, it’s possible that >60% of the risk is modifiable. What about the remaining % though? ![]()
Do we know what they consider “high” LDL?
Thanks a lot!
They cite “A study of 1 189 090 participants reported that high LDL cholesterol (ie, >3 mmol/L) was associated with an increased risk of dementia (HR 1·33, 95% CI 1·26–1·41).” (3 mmol/L = 116 mg/dL)
For hypertension, they use 130 mmHg!
Prevent or reduce hypertension and maintain systolic blood pressure of 130 mm Hg or less from age 40 years.
Other interesting bits:
Some evidence suggests that people taking some types of anti-diabetic medication might be less at risk of dementia. A systematic review, meta-analysis, and network analysis of 27 studies (1 590 757 participants), which did not report heterogeneity, identified that cohort studies indicated that SGLT2 inhibitors (OR 0·41, 95% CI 0·22–0·76), GLP-1 receptor agonists (0·34, 0·14–0·85), and DPP-4 inhibitors (0·78, 0·61–0·99) were associated with dementia risk reduction, whereas sulfonylureas were associated with increased risk (1·43, 1·11–1·82).186 Metformin was not associated with a decreased or increased risk (0·71, 0·46–1·08).
Overall improved control of diabetes, but not very low blood sugar or weight loss without improved diabetic control, might attenuate the risk of dementia and be a way of decreasing dementia risk.
On BPV:
These meta-analyses did not cover blood pressure variability, but a cohort study (n=2234; aged ≥65 years) measured blood pressure variability with assessments over 3, 6, 9, and 12 years and reported that each unit increase in systolic variability was associated with increased risk of dementia, with HRs ranging from 1·02 (95% CI 1·01–1·04) to 1·10 (1·05–1·16).
On depression:
People who were treated for depression by pharmacotherapy (n=14 695; 0·77, 0·65–0·91), psychotherapy (n=2151; 0·74, 0·58–0·94), or combination therapy (n=5281; 0·62, 0·53–0·73) were less likely to develop dementia than the untreated group (overall treatment HR 0·69, 0·62–0·77). The untreated group who remitted did not have a higher risk of dementia than the group without depression (0·84, 0·56–1·24).
The findings on the effect of medication and therapy for depression in reducing the risk of dementia suggest the importance of treating depression both for quality of life and because it might reduce the risk of dementia in the future.
We previously described the evidence that antidepressants are no more effective than placebo for depression in people with dementia.
In “Potential risk factors considered with insufficient evidence to include in the model” they included:
Nothing new for people here, but it’s good that these conclusions slowly reach the mainstream.
Kaiser (a large HMO in CA) considers systolic bp >130mm HG as Stage 1 hypertension.
Unfortunately, the less educated is really reaching. I know so many professors, doctors and professionals who once they reached 80 Are showing signs of dementia. The science community continues to reach for answers. Are we really that much closer to a cure?
I think the less educated is a very reasonable call. They are only saying a 5% increase by having less education. However, because the data in is crappy, the data out isn’t specific enough.
I’d be much more interested in effects and correlations between those who are high utilizers of their brains for complex tasks with high frequency, and those who don’t use their brain’s much. I suspect the lower education might partially be a proxy for this -but I’d expect a more powerful effect.
I’d also like to see stats if they looked at optimal BP, ApoB, Omega 3 index, Vitamin D, HbA1C of <5. I suspect there is a more potent effect to be seen by optimizing.
Yes they follow the American guidelines. But the European and International guidelines use 140 mmHg as the threshold. So it’s interesting that the international commission on dementia prevention used 130 and not 140.
I did not realize European and Intl guidelines for hypertension were higher…thanks!
NYTimes article published today about prevention that references the Lancet Report. The link should work for those without access to NYTimes. The 10 “tips” given are so simple and easy to put into action. But generally, don’t get a brain injury as they are not reversible.
Small tweaks to your daily routine can go a long way toward protecting your body’s control center and preventing cognitive decline down the road. In fact, scientists believe that as many as 45 percent of dementia cases could be delayed or prevented with help from some simple, sometimes surprising, changes in behavior.
It’s never too early or too late to start, but time is of the essence when it comes to building your brain’s defenses, especially since it’s generally impossible to reverse brain damage once it’s happened, said Dr. Eva Feldman, a professor of neurology at the University of Michigan’s Neuroscience Institute.
We asked eight neurologists and neuroscientists to share their best tips.