I saw @DrFraser 's post on DSIP earlier, so wanted to learn more about this peptide:
Some interesting points:
Despite its early promise, DSIP remains an enigma in modern molecular biology—often referred to as an “orphan” peptide. Unlike other neuropeptides such as ghrelin or oxytocin, for which specific genes and high-affinity receptors have been cloned and characterized, the genomic origin of DSIP and its specific receptor target remain elusive in the human genome. This “orphan” status has created a dichotomy in the scientific community: while empirical evidence from animal models and human clinical trials in the 1980s demonstrated significant therapeutic potential, particularly in addiction and stress management, the lack of a defined molecular pathway has stalled its development into a licensed pharmaceutical agent.
This report provides an exhaustive analysis of the scientific and clinical landscape of DSIP. It synthesizes data from early foundational studies to the most recent 2024 investigations into fusion peptides, examining the peptide’s biochemistry, its controversial but documented effects on sleep and hormones, and the regulatory challenges that currently define its status as an unauthorized substance in major jurisdictions.
Implications of the DSIP-GILZ Connection:
Stress Resilience: The GILZ protein is upregulated by dexamethasone (a potent corticosteroid) as a negative feedback mechanism to control inflammation. If DSIP functions similarly, it acts as a physiological “brake” on the stress response, preventing the deleterious effects of chronic cortisol exposure.
Gene Regulation: Research indicates that DSIP can influence the expression of early response genes (c-Fos/c-Jun), which are downstream targets of the MAPK pathway. This supports the view of DSIP as a “programmer” of genomic expression rather than a simple neurotransmitter agonist.
Modulation of Neurotransmitter Systems
DSIP does not appear to act as a direct ligand for a single neurotransmitter receptor (like a key in a lock). Instead, it functions as a neuromodulator, altering the baseline activity of multiple systems to favor a state of rest and homeostasis.
GABAergic System: The peptide has been shown to potentiate the activity of the Gamma-Aminobutyric Acid (GABA) system, the primary inhibitory network in the mammalian brain. This activation is likely responsible for its anticonvulsant and anxiolytic properties.
NMDA/Glutamate: There is evidence of interaction with N-methyl-D-aspartate (NMDA) receptors, helping to balance excitatory glutamatergic transmission. By curbing excessive glutamate activity, DSIP may protect neurons from excitotoxicity, a mechanism relevant to its benefits in alcohol withdrawal (where glutamate rebound is a primary cause of seizures).
Opioid Receptors: While not a classic opioid, DSIP exhibits agonistic activity on opioid receptors or modulates endogenous opioid peptides (enkephalins/endorphins). This interaction underpins its potent effects in mitigating opiate withdrawal symptoms.
Serotonin and Dopamine: In models of insomnia, DSIP administration has been observed to restore depleted levels of serotonin (5-HT) and dopamine, correcting the neurochemical imbalances driven by sleep deprivation.
The “Bell-Shaped” Dose Response
A consistent finding in DSIP research is its non-linear, “bell-shaped” dose-response curve (an inverted U-curve). Lower, physiological doses often produce significant effects on sleep and hormonal regulation, while higher, supraphysiological doses may show diminished or even paradoxical effects. This characteristic is typical of hormetic substances and regulatory peptides, suggesting that DSIP works by triggering a cascade or signaling a threshold rather than by mass-action binding. This property also complicates clinical dosing, as “more” is not necessarily “better”.
Historical Clinical Trials (1980s)
The most direct evidence for DSIP as a sleep therapeutic comes from a series of clinical trials conducted in the late 1970s and early 1980s. These studies were unique in that they evaluated the peptide in humans with severe sleep pathologies.
Chronic Insomnia: In an open-label study involving patients with severe chronic insomnia, a treatment regimen of 10 intravenous injections of DSIP (25 nmol/kg) resulted in a normalization of sleep patterns that persisted for follow-up periods of 3 to 7 months.Crucially, the patients reported not just improved sleep duration, but improved daytime mood and performance, distinguishing DSIP from benzodiazepines which often cause daytime drowsiness and cognitive impairment.
Narcolepsy: A case study of a 35-year-old male with narcolepsy demonstrated that repeated DSIP injections reduced the frequency of uncontrollable sleep attacks (cataplexy/hypersomnia) and increased daytime alertness. Polysomnography revealed that DSIP “compressed” the sleep period, enhancing the efficiency of REM sleep and accentuating the natural circadian rhythm. This suggests DSIP acts as a chronobiological organizer.
Sleep Pressure and Architecture: In healthy volunteers, DSIP injection generated a feeling of “sleep pressure” (the natural urge to sleep) within 130 minutes. Total sleep time increased by 59% compared to placebo. The EEG analysis showed a reduction in Stage 1 (light) sleep and better sleep efficiency, with no evidence of pharmacological sedation. This supports the hypothesis that DSIP sustains natural sleep mechanisms rather than inducing an artificial coma-like state.
Implications for Testosterone and Fertility
While direct human clinical trials measuring testosterone elevation solely from DSIP are rare, the mechanism (Increased LHRH > Increased LH > Increased Testosterone) is physiologically sound.
Restoration: DSIP is clinically relevant for secondary hypogonadism induced by stress or sleep deprivation. Since the majority of testosterone release occurs during Slow-Wave Sleep (SWS), DSIP’s dual action of enhancing SWS and directly stimulating LHRH creates a synergistic environment for hormonal recovery.11
Puberty and Development: The finding that DSIP levels and LH release both increase during sleep in puberty suggests the peptide may play a natural physiological role in the developmental surge of reproductive hormones.23
Cytoprotection, Anti-Aging, and Pain Management
7.1 Antioxidant and Mitochondrial Effects
Beyond the brain, DSIP exhibits systemic cytoprotective properties.
Oxidative Phosphorylation: It enhances the efficiency of oxidative phosphorylation in mitochondria, optimizing energy production while minimizing the leakage of free radicals.
Enzymatic Defense: A 2011 study confirmed that DSIP activates endogenous antioxidant enzymes, including superoxide dismutase (SOD) and glutathione peroxidase, conferring a “strong antioxidant effect” in rat models.
Lysosomal Stability: In a study of rats aged 2 to 24 months, DSIP administration stabilized lysosomal membranes in the brain, heart, and liver. Lysosomes are the waste disposal units of the cell; their instability leads to the accumulation of cellular debris (lipofuscin) associated with aging. By stabilizing these organelles, DSIP may retard cellular senescence.
The Safety Paradox: “Incredibly Safe” vs. “High Risk”
There is a distinct contradiction between the historical safety data of DSIP and its current regulatory classification.
Historical View: Early researchers described DSIP as “incredibly safe.” Animal studies failed to identify a lethal dose (LD50), and human trials reported no significant adverse events other than transient headaches or nausea.
Modern Regulatory View: The FDA has placed DSIP on the 503B Bulks List Category 2. This category is reserved for substances that present “Significant Safety Risks” and are prohibited from use in compounding.
The Immunogenicity Argument
The FDA’s primary objection to DSIP is the risk of immunogenicity.
The Theory: Peptide drugs can be recognized by the immune system as foreign antigens. This can lead to the production of Anti-Drug Antibodies (ADAs).
The Danger: If the body creates antibodies against exogenous DSIP, these antibodies might cross-react with endogenous DSIP (or DSIP-like proteins/GILZ). This could theoretically lead to a deficiency syndrome where the body neutralizes its own sleep/stress regulatory factors, potentially causing autoimmunity or hypersensitivity reactions.
Evidence: The FDA notes that “no safety-related information” regarding immunogenicity has been identified to disprove this risk. Essentially, the lack of modern data proving it doesn’t happen is the reason for the restriction.
I’m glad you started this. I, too, noticed his post and have already been asking around.
One person let me know they did not see much of a benefit when using it as a nasal spray. It appears that sub q is most likely the way to go. For something you need to do before bed, that would be less convenient for many.
On one of the forums I read someone questioning if LDN might make it inactive because they both work on the opioid receptors.
It’s a relatively inexpensive peptide to purchase. I also read that the standard dosage ranges from 100-250 mcg.
I remember when I first started looking into DSIP around 2019, I saw far too many anecdotes from people saying it actually made their sleep worse. I tried it anyway and didn’t notice anything.
My question here is did you have a good sleep phase monitor that lists REM, Deep Sleep, etc? I’m not sure if you’ll necessarily notice anything by having more deep sleep. Also, I suspect this doesn’t work for everyone, but the 2 people who just started it that I do, the data is pretty consistent. There will be more to follow and I’ll get more data.
DSIP is one of those peptides that sounds exciting but has a reputation for being very hit or miss - I see more misses than hits - and like @LukeMV said, some people get worse. Peptide protocol pioneer Chris Duffin is one of the latter.
These comments are from skool.com groups (free). Anthony Castore is an authority on peptides.
Pinealon and Epitalon produce more consistently positive reports.
I’ve had a sleep disorder for 20 years - what has worked better than anything for me is Nootropics Depot Sensoril ashwaganda. The substantial RHR drop, HRV increase, and reduced awakenings were immediate and have persisted.
So in regard to sleep architecture Oura Ring or Eight Sleep Bed - we have both and they measure out very similarly.
Pinealon and Epitalon may indeed be superior for many individuals. I’ve seen no change with Epitalon, but I didn’t take it for more than a week and was using the dosing for a telomerase. I’ve not tried Penealon.
@AgentSmith what dosing do you use for these and are you using them in combination?
The beauty of being able to collect N=1 data is that one can try various options and objectively see the results. It is pretty hard to placebo effect up a consistent change in one’s sleep.
On average, my deep sleep has increased by ~65%, today it was the highest it has been at 30% (6.3 hrs x 0.3 = 1.9 hrs). This does come at a cost of a very slight decrease in my REM which is still very good - but I guess the additional time in deep sleep has to come from somewhere.
Also thanks @RapAdmin for the interesting write-up, learned a few things from that.
In the spirit of throwing everything against the wall for the husband…
Nootropics will arrive tomorrow, thank you!
Are there any negatives regarding safety you know of with pinealon and/or Epitalon?
From what I can see, dsip is perfectly safe. (I’ll order this too just to try incase it helps him)
My deep sleep is good (45-90 minutes), but it’s not a high percentage of sleep.
My over all sleep is phenomenal, but I’ll probably try DSIP just for the sake of science… I, too, have the mattress and ring to share data.
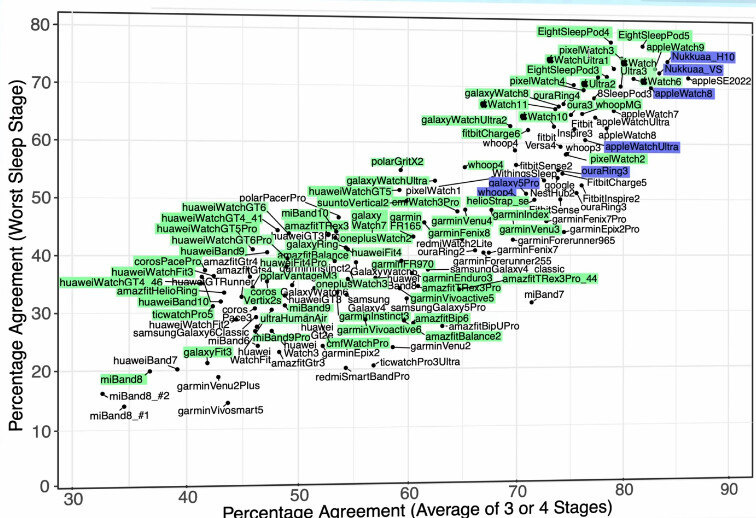
Here’s a graph from Quantified Scientist on best sleep trackers, apple watch apparently have had some problem with deep sleep tracking, but overall a few at the top: eight sleep pod, apple watch, oura ring, whoop. So for those of you who are wondering about which tracker to measure deep sleep most accurately.
I didn’t have a tracker, but I was having sleep issues (which is still true on occasion) and it didn’t help me fall asleep or stay asleep any better than before I started taking it.
I don’t think it necessarily is a sleeping medication - presuming it works at all (which I am growing to think it does). A lot of items that generate sleep often worsen sleep architecture in regard to adequate REM or Deep Sleep. If one needs such a medication to sleep - potentially do so with caution and with careful consideration of neurocognitive decline risks (benzos, ambien, and especially drugs with anticholinergic effects/older antihistamines).
However, if not using a medication, or if using a medication to get enough sleep, fall asleep and reinitiate sleep post waking, if your deep sleep is low - this could be an item worth trying. I think the only one of these items that DSIP seems to help is falling back asleep if one awakens - the rest I haven’t seen any change.
This is probably why individuals who try it for “sleep” might say it doesn’t work. If one is trying to generate more deep sleep, that will be something that will be measured and potentially not felt.
Additionally with the sleep monitors, at least on some of the discussions I’ve heard from the scientists at Oura are far from perfect, BUT the errors they have on an individual tend to be consistent, and the trends are quite reliable. So having a baseline deep and REM and doing something for a month and comparing if there are changes is probably the best way to utilize these tracking devices.
I had more success in with epitalon for staying asleep, vs dsip. I was using a nasal spray for both. I usually took them at night.
The best sleep I had was when I was on a ipamorelin / tesamorelin cycle. Didn’t matter when I took them. My recovery after workouts was really good while on this cycle.
The worst sleep I had was when I was on a gh cycle, 2iu. Didn’t matter when I took it, I felt rundown the next day.
I don’t doubt at all that DSIP is really working for you and your wife and some patients. It really seems to work quite well when it works. I am just relaying that the most common refrain on various forums is that it has no discernable effect. Given that it works so well for some people, and it is rather inexpensive, I would definitely recommend people try it.
I will say that once I did experience a 25% increase in deep sleep after using it, but it was only one night so I hesitated to attribute it to the peptide. But perhaps it was. I use Oura and Eight Sleep, but find that Oura seems much more accurate vs. my subjective assessment.
There is the issue of dosing and timing DSIP, of course. Maybe those of us not getting a benefit are using it incorrectly. I have tried various doses (100-300mcg), frequencies (daily, every other day, every 3rd day), and injection times (mid-morning, 1-2 hours before bed).
If there is a specific protocol that seems to work reliably, I will gladly try it again.
Epitalon I have used anywhere from 100mcg/day to 10mg/day (when I was new to peptides and was following bad advice!) for 2-3 weeks. I tend to use it once or twice a year. Pinealon I have not tried.
No negatives that I know of. People sometimes speculate about pinealon lowering the seizure threshold because one of the AAs is glutamate and it may impact neuroplasticity, but there’s zero evidence for seizures in animal or Russian studies.
I think people need to find “my” dose with this one. Not unlike GLP1’s there is not one dose that fits all, even thought the max dose is pretty consistent for all, still not all need the max dose to be successful.
Again, like GLP1’s this one is fairly easy to measure a result, instead of the scale being your friend, a good sleep tracker that provides info on duration, deep sleep and REM will tell the tale. If you have not used a sleep tracker, get one before you start DSIP and use it for 2 weeks to get a baseline.
We started at 250 mcg, every night just before bed, same time we’ve been taking our Ipa + CJC combo for the past 2 years.
After a week, a small difference so upped to to 350mcg for 2 weeks and had a better response then went up to 400mcg and that was our sweet spot.
We both have experienced “consolidation” of our DS cycles and increased time in DS.
Consolidation means our DS cycles happen closer together instead of being scattered thought the entire sleep cycle, and interrupting REM later in the sleep cycle. This is one of the effects that is considered beneficial, beside the increase of DS.
DSIP does not work that way, it does only 2 things, 1) consolidate DS and 2) increase the amount of DS.
It is not a sleep aid, does not make you sleepy, and does not have any after effects, all it does is increase the quality of your DS.
Which increase I would never have noticed, without a sleep tracker as I do not feel much different (sleep is my super power) but I do understand the benefit of increased DS that helps the glymphatic system in clearing out the detritus in the brain while we sleep. And that is why it is in my permanent peptide regimen.
Happy 2026 Everyone!
I’m just here to share my initial experience on with DSIP
First night I took 100mcg and had 1:10 of deep sleep, 15%
Last night I took 250mcg and had 1:00 of deep sleep, 12%
These are very typical numbers. For perspective, the night before I took any, I had 1:38 deep sleep 21% and the night before that was 1:38 at 18%
I did have a particularly good night of sleep last night, but that could easily be my normal fluctuation.
I’ll come back and edit this as I get more results (is editing the same post the best way to go about it?).
EDIT:
Night 3 I took aprox 400mcg of DSIP and my deep sleep was 1:01 13%
So, thus far, it seems this doesn’t do anything for me?? @Steve_Combi at what point does one give up?