If there is a “silver bullet” in the longevity pharmacopeia, this review confirms it is Rapamycin. In a field often plagued by hype and unreplicable results, the inhibition of the Mechanistic Target of Rapamycin (mTOR) stands apart as the only intervention with a near-perfect batting average across every model organism tested. This 2025 review serves as a definitive dossier, arguing that we have moved past asking if mTOR inhibition works, and must now focus on how to deploy it for maximum benefit in humans.
The authors detail how hyperactive mTOR signaling is the central engine of aging—driving cellular senescence (“zombie cells”) and blocking repair. By inhibiting this pathway, Rapamycin flips a genetic switch from “growth at all costs” to “maintenance and repair,” effectively mimicking the profound benefits of calorie restriction without the metabolic misery. Most critically for humans, the data shows that intervention in late life is still effective, reversing age-related decline even when started in the biological equivalent of a 60-year-old. The message is clear: It is not too late to slow the clock.
Source Review Paper:
Institution: Shoolini University, VSB-Technical University of Ostrava, et al. (International Consortium).
Country: India / Czech Republic / Slovakia.
Journal Name: EXCLI Journal.
Impact Factor: 4.9 (Significant impact in experimental clinical sciences).
Part 2: The Biohacker Analysis
Study Design Specifications
Type:Systematic Review & Meta-Analysis of the “Gold Standard” literature.
Subjects: Complete evolutionary spectrum: Yeast (S. cerevisiae), Worms (C. elegans), Flies (D. melanogaster), and Mice (M. musculus).
Lifespan Data (The “Upside”):
Yeast: Chronological lifespan extended by ~54%.
Worms: Median lifespan extension of ~19%.
Flies: Females show up to 23% maximum lifespan extension.
Mice: The most compelling data for humans.
Consistency: Reproducible extension of 10-18% across genetically diverse strains (unlike other compounds that fail in heterogeneous groups).
Late-Onset Efficacy: Treatment started at 20 months (old age) still extended remaining lifespan significantly.
Mechanistic Deep Dive: The Engine of Youth
The review confirms that mTOR inhibition is not merely slowing damage accumulation; it is actively restoring youthful cellular function through three key pathways:
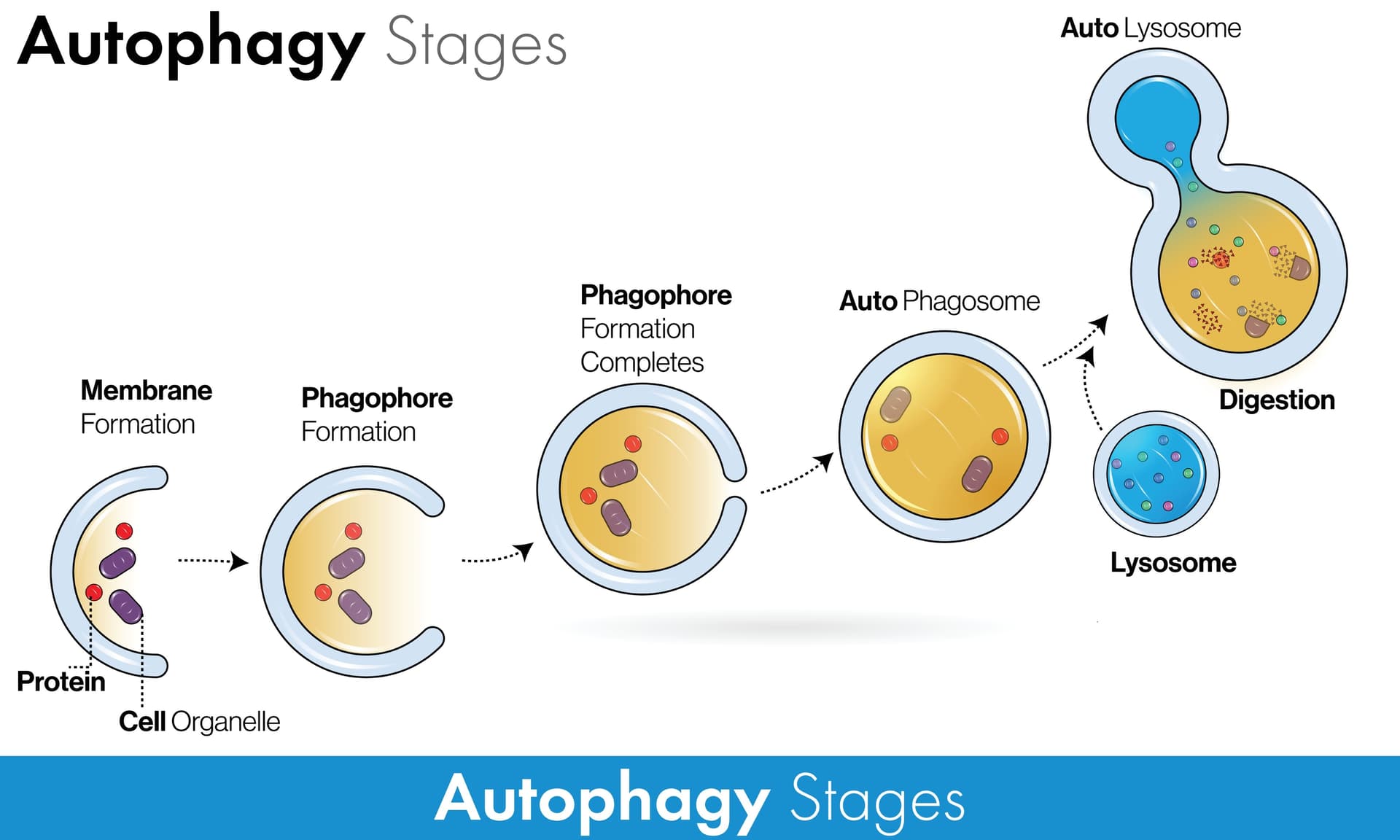
Restoration of Autophagy:
The Mechanism: mTORC1 naturally inhibits autophagy. Rapamycin releases this brake.
The Benefit: This triggers the cellular “clean-up crew,” digesting misfolded proteins (Alzheimer’s plaques) and dysfunctional mitochondria. This is the primary driver of the anti-aging effect.
The Mechanism: Instead of just killing senescent cells (senolytics), mTOR inhibition suppresses their ability to secrete inflammatory signals (the SASP).
The Benefit: This dramatically reduces systemic inflammation (“inflammaging”) without destroying the tissue architecture.
Stem Cell Preservation:
The Mechanism: By preventing stem cell exhaustion (hyper-proliferation), rapamycin maintains the regenerative pool.
The Benefit: Enhanced wound healing and tissue maintenance in the long term, contrary to the fear that it stops growth.
Novelty
This paper solidifies the transition of Rapamycin from an “immunosuppressant” to an “immunomodulator.” The authors present data showing that while high doses suppress immunity, longevity-associated doses actually rejuvenate the immune system in the elderly (likely by clearing senescent immune cells), improving response to vaccines and infection—a massive paradigm shift.
Critical Limitations (The Engineering Challenge)
The Dosage Puzzle: The “toxicity” often cited is a result of continuous dosing (transplant protocols). The paper implies, but does not solve, that the key to avoiding side effects is pulsed dosing.
Glucose dysregulation: The review notes hyperglycemia in some models, but newer interpretations suggest this may be “starvation diabetes” (a benign physiological shift to fat oxidation) rather than pathological insulin resistance.
Part 3: Actionable Intelligence
The Protocol: The “Bull Case” Translation
Strategy:High-Dose Intermittent (Pulse) Therapy.
Rationale: Maximize mTORC1 inhibition (autophagy trigger) while allowing mTORC2 recovery (safety) during the off-days.
Protocol:5mg – 8mg of Rapamycin (Sirolimus) taken once weekly.
Absorption Hack: Take with a high-fat meal (e.g., olive oil, avocado) to increase bioavailability by up to 30%, getting more “bang for your buck.”
The “Stack”: Pair with Acarbose (to blunt glucose spikes) or Glycine (to support methylation).
Biomarkers: Optimization Metrics
Don’t just look for toxicity; look for efficacy:
Inflammation: Target an hs-CRP < 0.5 mg/L. Rapamycin is a potent anti-inflammatory; a drop here is a sign of success.
Biological Age Clocks: If available (DNAmGrimAge), track the deceleration of epigenetic aging.
HOMA-IR: Monitor insulin resistance. If it creeps up, adjust the pulse frequency (e.g., once every 10 days instead of 7) rather than quitting.
Feasibility & ROI
Cost-Benefit:Extreme Value. Generic Sirolimus is relatively inexpensive ($1-$3 per mg).
ROI: Compared to unproven supplements (NMN, Resveratrol) which cost hundreds monthly for marginal/placebo gains, Rapamycin offers the highest probability of genuine biological age reversal for the dollar.
Population Applicability
Broad Spectrum: Unlike interventions that require specific genetic makeups, the conservation of the mTOR pathway implies this will work for the vast majority of humans.
Target Demographic: Ideally suited for individuals 40+, where natural autophagy begins to decline precipitously.
I’ve been reading and researching a bit in last few days, and it seems the best results on Longevity are when rapa is combined with metformin (and maybe SGLT2’s) and since i already take metformin and SGLT2 daily/nightly what would you guys think of doing a daily dose of Rapa (maybe 1MG with EEVO) to get the combined Rapa+Metformin benefits?
While I know many are worried about the Mtorc2, but I would be willing to sacrifice it and see how it goes for while? Has any of you guys tried it this way? and what do you think in general (again ignoring the effect on mtorc2 for now)
A few people here have tried it and do it still (I think). I avoid metformin generally (except periodically when I’m not exercising) due to the negative impact on exercise adaptions in muscles. And the mTORC2 inhibition is something highly personal, some people see reactions (blood glucose, lipids dis regulation, etc.) at daily low doses, but I’ve dosed up to 30mg and no issues generally (some lipid disreg. at higher weekly doses), but fully controlled with other lipid medications.
I don’t view dosing experiments as anything other than that. I’m always trying different doses and tracking results with blood tests. We all have to figure out what works best for our bodies and genes.
Thanks @RapAdmin for the great info and references. I hear you about metformin and exercise, but It doesn’t seem to affect me much (with the caveat that I do moderate exercise, and don’t like to push the limits, so have not seen a change while on metformin) plus I’ve seen renewed interest on metformin (as a longevity substance) lately so I’ve decided to continue with it, though at a somewhat lower dose (500mg) since I also do either Empa or Cana.
I agree with experimenting (while being careful and watching the markers) and seeing what works best at individual level.
So, starting tonight my experiment will start with daily Rapa and Metformin plus any other meds I already take.
will come here and update after couple months when I run some testing.
r.e. I’m starting to think that most supplements (save three-four of them, i.e. magnesium, vitD, Glycine, maybe boron for males and couple can’t remember now) have little to no effect on longevity which kind of sucks as I have stacks of so many to last me year’s LOL.
My money is on repurposed meds for now (as opposed to supplements).
RapAdmin,
Unless its already being done, is there a way to organize these publications (some of which can be considered seminal) to organize into a master library folder as opppsed to general discussion threads where they get buried into enormous amounts of info added everu single day. I try to book mark them for easy access but thats an individuallstic approach.
Combining metformin with high-intensity exercise interferes with improvements in VO₂ max and vascular insulin sensitivity. Adults performing low- or high-intensity aerobic exercise for 16 weeks while taking metformin (2,000 mg/day) showed no improvement in VO₂ max. Those on placebo improved by about 6% on average. Metformin also blunted increases in macrovascular and microvascular insulin sensitivity seen with both exercise intensities, attenuated improvements in fasting blood glucose, and prevented gains in whole-body insulin sensitivity, even after high-intensity exercise. This is not isolated; other trials show metformin interferes with multiple exercise adaptations, likely via inhibition of mitochondrial complex I, which disrupts cellular energy sensing. Metformin remains an excellent, safe first-line therapy for type 2 diabetes. But caution is warranted when using it as a general “longevity drug” in healthy, active people, especially if it interferes with the single most powerful longevity intervention we have, exercise.
Regarding the above statement: The statement you provided is a direct summary of findings from a study published in October 2025 by Steven K. Malin and colleagues at Rutgers University, likely combined with context from earlier mechanistic work by Adam R. Konopka.
Protocol: 16 weeks of supervised aerobic exercise.
Dose: 2,000 mg/day of Metformin vs. Placebo.
Groups: Randomized to Low-Intensity or High-Intensity aerobic exercise.
The Findings:
VO₂ Max: Placebo group improved; Metformin group showed no improvement in VO₂ max regardless of intensity.
Vascular Insulin Sensitivity: Exercise improved microvascular and macrovascular insulin sensitivity in the placebo group, but Metformin blunted these improvements.
Glucose: Metformin attenuated the reductions in fasting blood glucose typically driven by exercise.
2. The Mechanistic Source (Mitochondrial Inhibition)
The text mentions: “likely via inhibition of mitochondrial complex I, which disrupts cellular energy sensing.”
This paper is the definitive mechanistic study demonstrating that Metformin inhibits skeletal muscle mitochondrial respiration (specifically Complex I), thereby preventing the hormetic stress response required for mitochondrial biogenesis and VO₂ max improvement.
Analysis of the Conflict: Metformin vs. Exercise
This data reinforces the “blunting hypothesis”—the idea that potent antioxidants or metabolic regulators (like Metformin) can neutralize the acute oxidative stress (ROS) and energy signals (AMPK activation) necessary for exercise adaptation.
Adaptation Metric
Exercise Only (Placebo)
Exercise + Metformin (2g/day)
Implication
VO₂ Max
Increased (~6%)
No Change
Metformin negated aerobic capacity gains, a critical predictor of all-cause mortality.
Vascular Function
Improved
Blunted
The drug prevented exercise-induced improvements in blood flow and endothelial function.
Insulin Sensitivity
Improved
Attenuated
While Metformin improves insulin sensitivity in sedentary diabetics, it appears to cap the “ceiling” of improvement possible through exercise in active individuals.
Longevity Context
For a healthy, active individual (non-diabetic), using Metformin as a “geroprotector” is increasingly difficult to justify based on this data.
The Trade-off: You are trading the single most potent longevity intervention (VO₂ max and mitochondrial density) for a theoretical reduction in aging pathways (mTOR inhibition) that exercise already modulates effectively.
The Risk: By inhibiting Complex I, Metformin creates a “low energy” signal that mimics caloric restriction, but when combined with the high energy demand of exercise, it causes metabolic interference rather than synergy.
Recommended Next Step
Since you are interested in longevity compounds, would you like me to compare Rapamycin or SGLT2 inhibitors (e.g., Canagliflozin) against this data to see if they share the same exercise-blunting profile?
Based on current clinical data and mechanistic studies, SGLT2 inhibitors and Pioglitazone do not share the exercise-blunting profile of Metformin. In fact, they may act synergistically with exercise.
GLP-1 receptor agonists, however, present a different set of challenges—specifically regarding muscle preservation—which can indirectly cap VO₂ max gains.
Here is the comparative analysis against the Metformin “blunting” data.
Verdict:Synergistic / Pro-Longevity
Unlike Metformin, SGLT2 inhibitors do not inhibit mitochondrial respiration. Evidence suggests they may enhance the benefits of exercise.
Mechanism: They induce a fasting-like state (increasing glucagon, reducing insulin) and promote ketone production (beta-hydroxybutyrate), which serves as a highly efficient fuel for cardiac and skeletal muscle.
Exercise Interaction:
VO₂ Max: Clinical trials (e.g., in heart failure and metabolic syndrome) show SGLT2 inhibitors improve peak VO₂ (~1.1 to 2.0 mL/kg/min increases) rather than blunting it.
Mitochondria: They appear to improve mitochondrial energetics by reducing cytosolic sodium and enhancing oxidative metabolism.
Longevity Note: This class is currently the strongest candidate for a “mimetic” that works alongside exercise rather than fighting it.
2. Pioglitazone (Thiazolidinediones)
Verdict:Mechanistically Synergistic (but with side effects)
Pioglitazone is mechanistically the “anti-Metformin” regarding mitochondria. While Metformin inhibits Complex I, Pioglitazone activates PPAR-γ, a nuclear receptor that drives mitochondrial biogenesis.
Mechanism: It upregulates PGC-1α, the “master regulator” of mitochondrial biogenesis—the exact same pathway activated by endurance exercise.
Exercise Interaction:
VO₂ Max: Studies indicate Pioglitazone can augment exercise-induced improvements in insulin sensitivity and VO₂ max.
Muscle: It reduces intramuscular fat (improving quality) but does not block hypertrophy signaling.
The Catch: While excellent for mitochondrial density, it causes fluid retention and subcutaneous fat gain, which can mechanically hinder performance even if cellular energetics are improved.
Verdict:Indirect Interference (Hardware degradation)
These drugs do not chemically “blunt” the signaling pathways (like AMPK or mTOR) in the same way Metformin does, but they pose a structural risk to VO₂ max.
Mechanism: Potent appetite suppression and insulin modulation.
Exercise Interaction:
VO₂ Max: Recent data shows that despite massive weight loss, VO₂ max (absolute) often decreases or stays flat. Relative VO₂ max (per kg) improves simply because the patient is lighter, not because cardiovascular fitness increased.
The Risk: Up to 40% of weight lost on GLP-1s can be lean tissue (muscle). By degrading the “hardware” (skeletal muscle mass) required to utilize oxygen, you may blunt the capacity for high-intensity output, even if mitochondrial function remains intact.
Summary: Interaction with Exercise Adaptation
Compound
Mitochondrial Impact
VO₂ Max Effect
Hypertrophy Risk
Longevity Verdict
Metformin
Inhibits Complex I (Blunts signal)
Blunted / No Gain
Inhibits mTOR (Blunts muscle growth)
Caution in active, healthy adults.
SGLT2 Inhibitors
Neutral / Enhancing (Ketosis)
Improved
Neutral
Top Tier adjunct to exercise.
Pioglitazone
Stimulates Biogenesis (PPAR-γ)
Augmented
Neutral (but fat gain risk)
Good specifically for mitochondrial poor responders.
GLP-1 RAs
Neutral
Mixed (often lower absolute VO₂)
High Risk (Sarcopenia)
Requires heavy resistance training to offset muscle loss.
Practical Implication for Longevity
If your goal is to maximize Healthspan (which is highly correlated with VO₂ max and muscle mass):
Avoid: Taking Metformin on the days you perform Zone 2 cardio or HIIT, or avoid it entirely if you are metabolically healthy (HbA1c < 5.7%).
Consider:SGLT2 inhibitors (like Canagliflozin/Empagliflozin) generally offer a safer profile for the “active extensionist.” They provide glucose control and mTOR modulation (indirectly via insulin lowering) without poisoning the mitochondrial electron transport chain.
Would you like me to detail a “cycling protocol” for these compounds that minimizes their interference with your specific training schedule?