As a type 1 diabetic who, despite “well controlled” blood sugars, will live a shorter life, this is incredibly exciting. Given that complications are largely a result of AGEs, therapies to reduce AGE formation has huge potential to improve long-term outcomes.
3 Likes
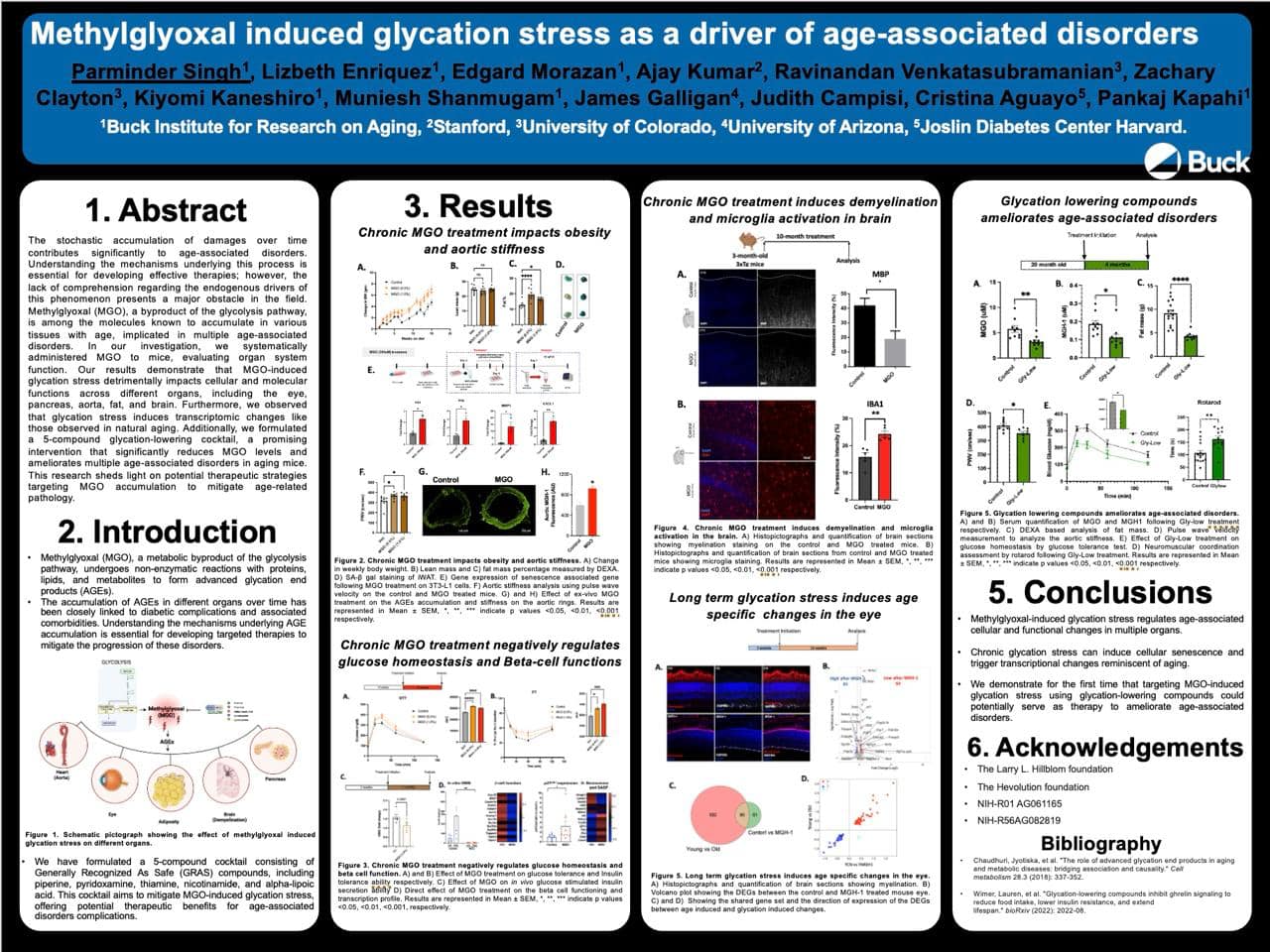
And another thread from Pankaj Kapahi of UCSF/Buck Institute:
Why not just use metformin+taurine as anti-glycation instead? That’s what Bryan Johnson uses, and many ppl are deficient in taurine
4 Likes
That’s cumulative running hours, so it looks to me like yellow makes all the gains in the first 30 hours. Mostly in the first 18. But, Yellow never really sleeps, which is kind of bad. The control sleeps 12 hours at a time.
I’m actually taking all the ingredients in GLYLO, in much greater quantities. And Rapa. Yet I never feel like running on a wheel.
3 Likes
What are the ingredients of GLYLO?
I may have spoken too soon. Unless I’m wrong that’s about a teaspoon of ground black pepper, and I may not get that much per day. Probably should buy that as a pill.
Didn’t somebody say that was a cyp3a inhibitor like GFJ? Probably not big enough to matter in the long run.
An update from Pankaj at the Buck Institute:
Looking forward to presenting our poster on how glycation lowering compounds can improve multiple aging outcomes. We will have multiple papers in the next 2 years - showing protection against insulin resistance, arterial function, eye aging, menopause, muscle function …. Not sure why it works against so many indications but the fact that GLYLO is a poly pill might be one reason
I agree, I’m convinced of the importance of melatonin on “genetic health”. One mechanism seems to be it’s impact on glutathione levels.
Another is re methylation
I’m sure there will be others.
BUT I’m wary of simply supplementing - because I assume this will down regulate endogenous production and so lead to dependency. So my approach is to focus on endogenous production - eat plenty of nuts, early daylight, consistent routine, warm white bulbs etc. But that may become insufficient at some point. As it is, i take melatonin only after drinking.
Very interested to hear how you determined dosage of melatonin and whether you’ve experiment with cycling/withdrawal
3 Likes
I agree with caution but with persistence in finding a solution. Melatonin production falls with age (correlation). I am working on my sleep and darkness hygiene but progress is slow with little ability to understand impact on indigenous melatonin production.
A work in progress to be sure.
2 Likes
I am quite experimental with melatonin and have built up to really quite high doses. I am, however, careful normally to only take it having initially slept for a while without using it. More recently I have been pleased to have at times slept for over 6 hours (as measured by fitbit ie ignoring waking periods) without melatonin and then used it to extend sleep for a hour or more.
I find 6 hours sleep duration (not 6 hours in bed) is sufficient for me to function fully (including writing computer programs or legal documents) for the next day without being tired. Hence I find it a good threshold. However, it can cause me not to sleep as well the next day as I am not as tired going to bed.
I also find melatonin a useful addition when I am drunk to reduce the effects of acetaldehyde. Combined with DHM, Pantethine and Molybdenum there is little space for acetaldehyde to impact on anything although there can be a sleep rebound.
I think dosing is quite a personal thing that people need to carefully work out for themselves potentially with medical advice as appropriate.
I would be interested in discussing experiences with anyone else trying really large doses, but I do not wish to encourage people to do that without taking advice.
I think the key point about Melatonin throughout the body is that it acts to reduce damage to mitochondrial DNA which is particularly vulnerable to ROS.
I thought people might like to see the melatonin that I use normally. These are 10mg, 12mg, 20mg and 60mg pills which can be taken to varying extents sublingually.

1 Like
“I assume this will down regulate endogenous production and so lead to dependency.”
There is no strong evidence that melatonin supplements shut down natural melatonin production, in fact, I can’t find a single relevant study. If you can find one I would be glad to read it.
FWIW:
I have been taking melatonin for over 40 years. It was the first “life-extending” supplement that I took based on the book “The Melatonin Miracle” by Walter Pierpaoli, M.D., Ph.D. and William Regelson, M.D.published by Simon and Schuster.
Walter Pierpaoli also published a book" Reversal of Aging: Resetting the Pineal Clock (Fourth Stromboli Conference on Aging and Cancer), Volume 1057, published by Wiley." he is still alive and well at age 89. Pierpaoli has published more than 140 papers in prestigious journals such as Nature etc.
I have been taking high doses of 100 mg+ for several months now with no negative results.
This was based on the self-experimenting with melatonin that @john_Hemming is doing.
Several times when traveling or on vacation I didn’t take any of my supplement stacks with me and it didn’t cause me to lose any sleep.
Melatonin in of itself does not cause drowsiness but merely sets or resets your biological clock.
4 Likes
You’re right. That was a lazy assumption on my part, that ill downgrade to a “concern”!
One thought though on high dosing: " Oral supplements can bring the levels of melatonin in the blood to levels much higher than is normally produced by the body. Dosages between 1 to 10 milligrams can raise melatonin concentrations to anywhere from 3 to 60 times typical levels"
Is there a particular logic to target super physiological levels?
One other thought - I’ve always been slightly horrified of pineal gland calcification. Other than maybe vit K2 (The biological responses of vitamin K2: A comprehensive review - PMC) is there anything else we should be doing to support this melatonin secreting gland?
I have been a fan of MK7 in avoiding calcification. I have made quite a bit of progress in working out the interplay between melatonin and the ultradian cycle linked to the HPA axis. However, it remains quite a complex system over all.
From my personal perspective the fact that I have expanded my natural sleep period (not every night) to be over 6 hours without melatonin is really good. I am not sure when I lost this, but it may have been 20 years ago.
1 Like
The papers are few and the evidence is still weak, but melatonin may have anti-cancer properties, especially breast cancer. Also, it may preserve the pineal gland and prevent age-related macular degeneration. Pierpaoli in his book thinks melatonin is anti-aging.
He also thinks that melatonin is not a true hormone.
I certainly do not advocate high-dose melatonin, it is just a self-experiment. At my age, I can afford to be a little more aggressive. As with rapamycin, my opinion is that younger people need smaller doses.
“Also the finding that melatonin seems to act on the hematopoietic activity of the bone marrow, combined with the separation of anti-proliferative, tumor-suppressive
agents in the bone marrow microenvironment, suggest an important link between pineal function, hemopoietic activity of the bone marrow, and circadian melatonin-related antiproliferative mechanisms in the bone marrow.”
Pierpaoli conducted pioneering research on melatonin and the pineal gland starting in the 1960s
He found melatonin production declines with age, leading to disrupted circadian rhythms
His research showed melatonin supplementation may help regulate circadian rhythms and sleep
He also found melatonin may have anti-aging and anticancer effects.
Effects of Melatonin in Age-Related
Macular Degeneration
https://sci-hub.se/10.1196/annals.1356.029
Melatonin: a principal neuroimmunoregulatory and
anti-stress hormone: its anti-aging effect
https://sci-hub.se/10.1016/0165-2478(87)90169-6
2 Likes
Chris Masterjohn mentioned there is increased mortality to those who megadose B vitamins (nicotinamide/niacin and thiamin and possibly riboflavin) which makes me more leery of this.
The main takeaway is that piperine is always good and I just got some from whole foods (need to get a larger glass jar from amazon if possible). And add loads of it to foods rich in B vitamins.
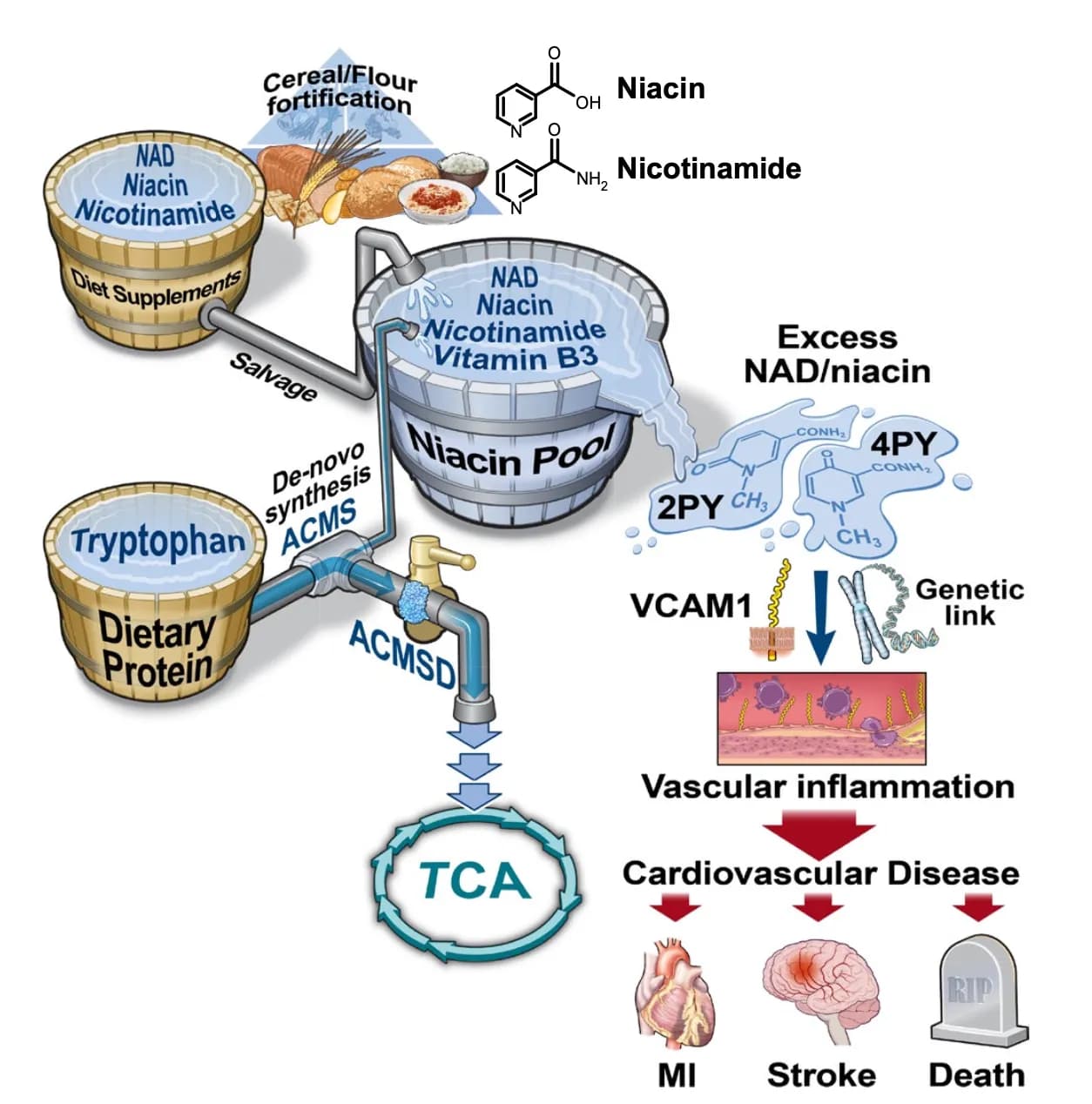
Without getting deep in the weeds there, I thought only Niacin was controversial whereas nicotinamide didn’t share the same putative side effects. Am I wrong?
1 Like
N’-methyl-4-pyridone-3-carboxamide (4-py) is the major metabolite of nicotinamide and nicotinic acid in rats. However, because it is complicated to determine 4-py in humans, there is only one report on its excretion. Recently we developed a method for the microdetermination of 4-py by high-performance liquid chromatography. Urinary excretion of 4-py in Japanese students from Teikoku Women’s University who consumed self-selected foods was 7.12 +/- 3.25 mumol/d, which is about one-fourth of N’-methylnicotinamide (MNA) and about one-ninth of N’-methyl-2-pyridone-5-carboxamide (2-py) excretion. The correlation coefficient between daily niacin equivalent (NE) intake and daily 4-py excretion was 0.529, which was about the same as the correlation coefficient between daily NE intake and daily 2-py excretion and which was two times higher than the correlation coefficient between daily NE intake and daily MNA excretion.
In rats, which are WAY more susceptible to 4PY
1 Like
Lots of noise.
1 Like